With the chaos and uncertainty at the federal level, New York Progressives see an opportunity to push for single-payer health care in the state – a plan that has been approved by the Democratic-controlled Assembly, but has been defeated by the Republican-controlled Senate (with the help of the so-called Independent Democratic coalition of state senators who were elected as Democrats but caucus with Republicans).
Irrespective of what Republicans do in Congress, Ron Widelec, a member of the steering committee of Long Island Activists (LongIslandActivists.org) said, “There is a lot we can do in New York – people forget we can act locally, not everything happens in Congress. Single payer is a real possibility in New York.”
Widelec exposed the lies that are used to beat back universal health care, despite the fact that every other industrialized nation has such a system:
That universal health care is too expensive, will add trillions of dollars to the national debt – but that is belied by the fact that the US spends twice as much on health care as any other industrialized nation, health care amounts to 1/6 of the entire economy, and the outcomes are poor, with the US ranked 32nd among nations, contradicting the claim that the US offers “the best health care in the world.”
Another lie is that universal health care will result in rationing, ”as if 20 million people with no insurance isn’t rationing, or people who have insurance but can’t afford deductibles or copays isn’t rationing, or insurance companies denying care isn’t rationing,” he said.
Janet Green, a nurse who lived in Canada for two years and now lives on Long Island, spoke of the difference: “We lived it, loved it – you could choose any doctor you like, be rid of billing, deductibles, copays; to be covered regardless of age, job status, preexisting conditions, personal wealth. No wonder the Canadians love their single payer universal health insurance system with private provision..
“When we moved to Long Island, the unfairness and inefficiency of an increasingly corporatized health care system was increasingly hard to take because I knew another system. I had coverage through husband’s job – but I was angry, not lucky, to be part of such an unfair system.” That included problems with doctors in/out network; merger/replacement of insurance plans, with changing rules, preferred provider lists not once but twice in 4 years. “There is none of that on single payer, no deductibles or copays or networks.
“I saw the misinformation spread by those most affected, the insurance industry –myths about Canadian system.
“North of the border and throughout the rest of the world, it is understood that to be a compassionate, enlightened society, there must be universal health coverage.
Dr. Martha Livingstone, vice chair of Physicians for a National Health Program, also spoke from experience about Canada’s health program, because she lived in Canada while getting one of her degrees.
“There are only two reasons we don’t have national health insurance Medicare for All – it is 1/6 of the economy and very powerful people are arrayed against us who will do everything in their power to persuade us we can’t have it. And our failure of imagination.
Indeed, it may well be that Republicans have overplayed their hand and the pendulum will swing back much more forcefully. If they succeed in repealing Obamacare and replacing it with Trumpcare, it can cost Republicans to lose Congress in 2018 and the White House in 2020, just as Obamacare cost Democrats control in 2010. Instead of Obamacare, which was Obama’s attempt to appease conservatives who demand a for-profit health care system, there will be universal health care, single-payer Medicare for All, a socialized health care system.
She told of a Victoria BC woman whose son had to go to five specialists before a rare brain tumor was diagnosed, treated, so he could survive. “In the states, he would have been one of 45,000 Americans dead of treatable medical conditions because he didn’t have access to timely medical care.
“Preexisting condition? Life is a preexisting condition, resulting from sexual contact and will invariable end in death. We all have a preexisting condition. We all need health care because we are human beings. How we will get it?
“We are the 99%. We don’t mind paying taxes when they provide for things we need. Who doesn’t want to pay taxes? it’s the billionaires – they want us to be uneducated, unhoused, unfed and if sick, they like us to die [and not be a burden on society]. It is a life/death fight.
“We have to protect the Affordable Care Act, but frankly my dears, ACA was written by the Heritage Foundation, a right wing think tank. It is a Republican plan first put into place by then Governor Mitt Romney in Massachusetts. You have piece a that‘s public, that funds the majority, and the piece that’s private.
“What Romneycare did, then ACA, was to build on the wildly expensive private for-profit sector of the system. We want to build in the wildly successful, inexpensively administered Medicare program…
“There are only two things wrong with Medicare: it doesn’t cover everything, doesn’t cover everybody. So improve it, Medicare for all.”
But regardless of what happens at the federal level, the state can create its own single-payer plan.
“Let New York be the first to have single-payer. What it will do for us in New York State is save us $50 billion, and save everybody but the very wealthiest New Yorkers money over what paying now for lousy access to care, where we have narrow networks, where some insurance genius can tell us at any moment, ‘Well, if you looked at p 793.’ The bill gets rid of all that – no copays, deductibles for a human right. We have to reinforce that. We know we won’t get it through the New York Senate this year, but 2018 if we hold their feet to the fire.”
“This event left me hopeful,” Widelec said before sending everyone off to their breakout sessions to come up with local actions. “The election of Trump wasn’t a hopeful time, but I am hopeful. I believe this is not a matter of left versus right, this is a matter of right versus wrong. One good thing about the 1%: we outnumber them 99 to 1.
Hundreds rallied at the Unitarian Universalist Fellowship of Huntington (UUFH), under the aegis of Long Island Activists, to strategize how to save Obamacare from Republicans who are moving swiftly to repeal it and replace it with something that is far more costly, would knock tens of millions off health insurance, would raise taxes for middle class and working Americans, and essentially be more costly for less care. But the Long Islanders went an extra step: to demand single-payer – that is, Medicare for All – beginning with New York State.
The rally was one of 150 across the country last weekend with some coordination of Bernie Sanders’ Our Revolution group.
The activists jammed a main room, overflowed the overflow room, and were lined up outside, producing a kind of echo-effect to cheers and boos inside the hall.
Long Island Activists rally for universal health care, Huntington, Long Island, Feb. 25, 2017.
“Something feels wrong. Public policy in no way reflects public opinion,” said Ron Widelec, a member of the steering committee of Long Island Activists (LongIslandActivists.org).
“We live in the richest country in history, yet 20 million go without health insurance, tens of millions have insurance but can’t afford to use because the deductibles so high – choosing between feeding children or going to a doctor when not feeling well. These are unacceptable choices in a country this wealthy…
“These are life-or-death situations. That’s why people are out here. It turns out, if you try to take away people’s health care, get angry and show up. Tens of thousands die without access to health care, or can’t afford access so that is the same as not having access. People die if they can’t afford an Epipen.
The Affordable Care Act (Obamacare) was not perfect because it was designed to appease conservatives. Indeed, the framework came out of the right-wing think tank, The Heritage Foundation, and was first implemented by Republican Governor Mitt Romney in Massachusetts. Elements such as a public option or a Medicare buy-in were omitted in order to satisfy so-called moderate Republicans like Susan Collins of Maine, who nonetheless voted against the ACA.
“Many members of Congress are dedicated to the idea they can make the situation even worse . Our position is clear: health care is a human right,” he declared to boisterous cheers.
“While no one thinks ACA perfect, it did things we need to fight for,” Widelec said. “ACA didn’t go far enough – a human right doesn’t have co-pays or deductibles.
“On the federal level, there is very little we can do with Congress. We know Republicans want to overthrow ACA… We have to fight to protect Obamacare and put pressure even on those too cowardly to hold town halls [like Long Island Congressmen Peter King and Lee Zeldin].
But while progressives all along wanted universal health care – that is, single-payer or what is termed Medicare for All – the most immediate goal is to preserve the key elements of Obamacare: covering young people on their parents’ plan until age 26; pre-existing conditions; no lifetime caps; a cap of no more than 20% of the premium going for non-patient spending , and minimal standards for what insurance policies cover – which turns out can only be offered if there is a mandate so that healthy people purchase insurance; otherwise, deductibles or copays or premiums are so high, they are unaffordable.
“It’s not true that the Republicans don’t have a plan,” warned Doreen DiLeonardo, who hosts a progressive radio show. Indeed, the plan that was exposed by Politico is essentially the 2015 bill introduced by then Congressman Tom Price, now the Secretary of Health & Human Services.
According to Politico, the Republican plan would rescind the unpopular individual mandate, subsidies based on people’s income, and all of the law’s taxes. It would significantly roll back Medicaid spending and give states money to create high risk pools for some people with pre-existing conditions. Instead of subsidies to help people with low incomes afford health insurance, it would give tax credits based on age rather than income. That means that multi-millionaire Rex Tillerson, former CEO of Exxon-Mobil and now Trump’s Secretary of State would get a bigger tax credit than the 30-year old who works at Starbucks. In any case, tax credits mainly benefit wealthier people. Meanwhile, the other big Republican idea is for Health Savings Accounts, which once again, benefit wealthier people, while those who are barely affording food and rent will be unable to stash away money in untaxed accounts. (See: Exclusive: Leaked GOP Obamacare replacement shrinks subsidies, Medicaid expansion)
What Democrats point to, though, are provisions that would wind up taxing middle class and working class families for the health insurance benefits they get from their employers, while at the same time ending taxes on the wealthiest Americans that funded the Obamacare subsidies.
“If it were such a good plan, they wouldn’t be hiding it,” DiLeonardo said.
The Republicans’ “destructive, nihilistic policy will ruin the ACA,” Assemblyman Charles Lavine, who has sponsored universal health care in the State Assembly, said. “They attempted to ruin it from beginning, based on lies. Each and every one here today, superheroesque, survivors of the ‘massacre at Bowling Green’, we know 20-30 million Americans would lose insurance, we know the tragedy that will flow from that – we will return to days preexisting conditions rob people of access to health care. You’re on your own. Lifetime caps – if someone had serious condition, cut off, no more insurance., – when that happens we all pay one way or another for their treatment. Women will pay more for identical coverage, young adults up to 26 no longer on parents’ coverage, you’re on your own.
“We know the lies being told. Trump said ACA robbed people of their insurance. We know that is just another lie. More than 20 million were able to get insured because of ACA, we now have a record low percentage of uninsured people, 10.9%.
“Trump said some plans were canceled [using this to accuse Obama of lying about ACA]. But that’s because they were deficient, illusory plans. What Trump and his confederates want to do, is to allow New Yorkers to go into market and buy insurance from other states. NYS is not going to allow that to happen. We will demand (because NY controls insurance product) that any insurance product sold here has to provide minimum requirements, or else people will get ripped off. Those are the kind of policies people lost because of ACA.”
Senator Chuck Grassley of Iowa lied when he said Obamacare would create death panels that would pull the plug on grandma. But a century ago, the worldwide flu epidemic killed off 50 to 100 million people, and bodies were piled up on street corners in Chicago waiting for the city to pick them up, people were on their own, too.
“That’s not that long ago – a blink in time of human history. We stand together you rebellious Americans to demand the human right of health care, and we stand together (big applause). This is a fight for our families, our communities. We are 36 years since the first days of Reagan Administration into a philosophy that says government isn’t the solution, it’s the problem, your enemy. You and I will fight for our families, communities, and damn well we stand up and fight for our government.”
Recalling that President Theodore Roosevelt, a progressive who busted up trusts and created the first national parks, whose home at Sagamore Hill is just a few miles from where this rally is taking place, Ron Widelec said, “Once republicans were progressives, put in policies that helped people, now they are wedded to the invisible hand of the American market, not noticing, it is a hand around throats of American people. We will fight back.”
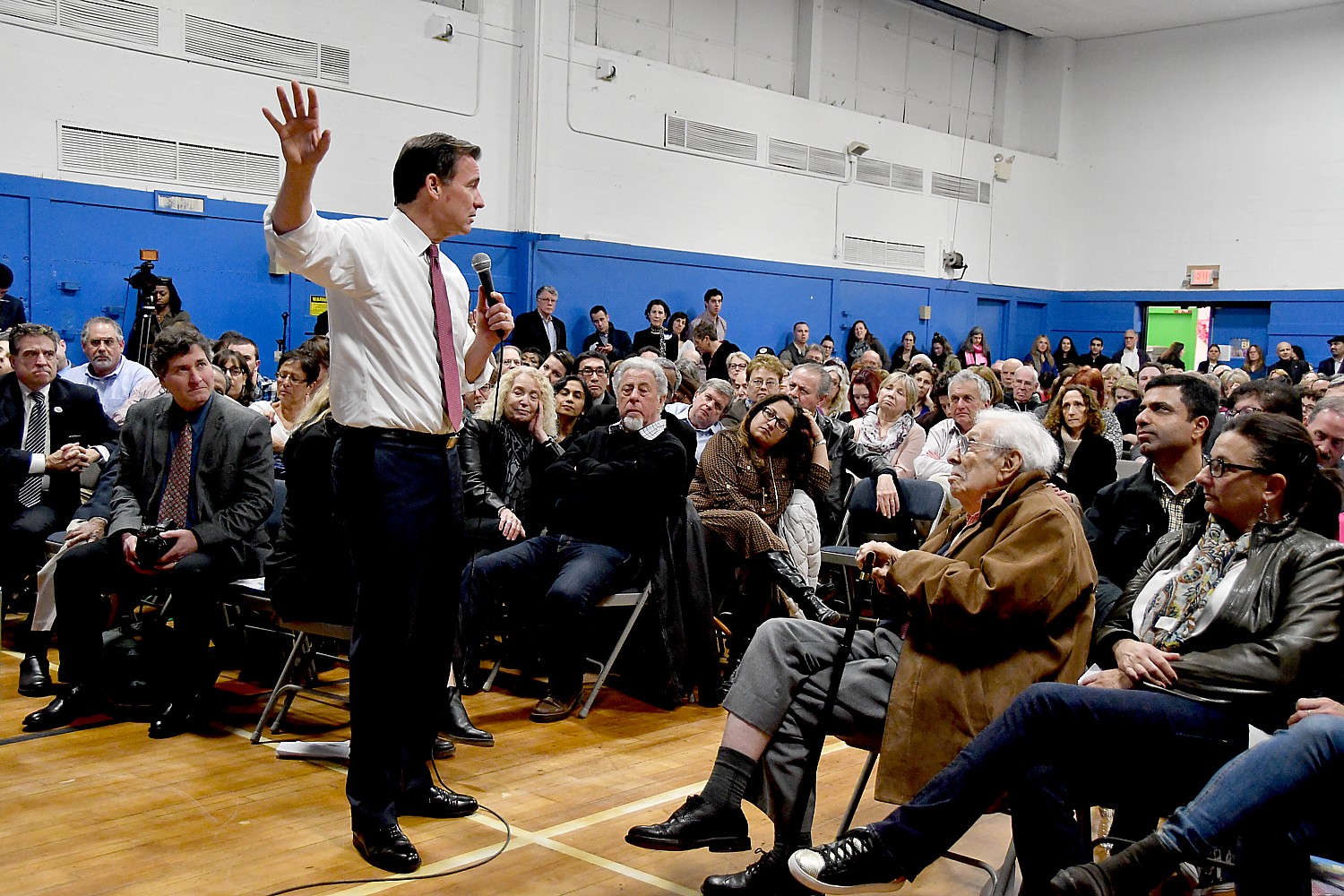
Newly elected Congressman Tom Suozzi, who has pledged to support universal health care once Democrats take back Congress (and held a packed town hall this past week in which support for ACA was a key issue), said “I believe in health care as a human right. This is a matter of life-and-death for many families now. We have to do a couple of things: protect ACA is the first thing. There is great energy behind that. But we need to improve upon ACA because there are problems – insurance companies, drug companies had too much say in writing ACA and we’re paying the price. Mend it don’t end it. Fix the problems.”
Next: New Yorkers Mobilize for Single Payer Health Care
Tom Suozzi’s town hall, his first as the Congressman representing New York’s 3rd District, was Standing Room Only, but he handled it with grace and aplomb, managing to organize what could have been an unruly outpouring of frustration, consternation, anger and anxiety into a productive discussion.
He presented the four key issues he believed most people wanted to discuss – Obamacare (Affordable Care Act), Trump-Putin ties and conflicts of interest, the travel ban, immigration and the environment – then held it up to a vote to ask if that met with approval. Then he picked four or five people to ask questions before moving on to the next topic.
Who wants to stay until 8:30? 9:15? 9:30? All night? 9:30 was the decision.
That’s how it went throughout the night with a return to key points: this is what democracy looks like. Let’s be realistic: I’m a junior Congressman from a minority party. And finally: it is up to you. Your voice. Your activism.
Most ingenious of all: he divided up his 3rd Congressional district into 16 neighborhoods – “The Third Will be Heard” – and tried to recruit people to join committees to stay active – write letters to local newspapers (the media with the most trust, he said), go door to door if necessary, engage in conversations with friends, family and others, instead of that old-saw of politics being a taboo subject.
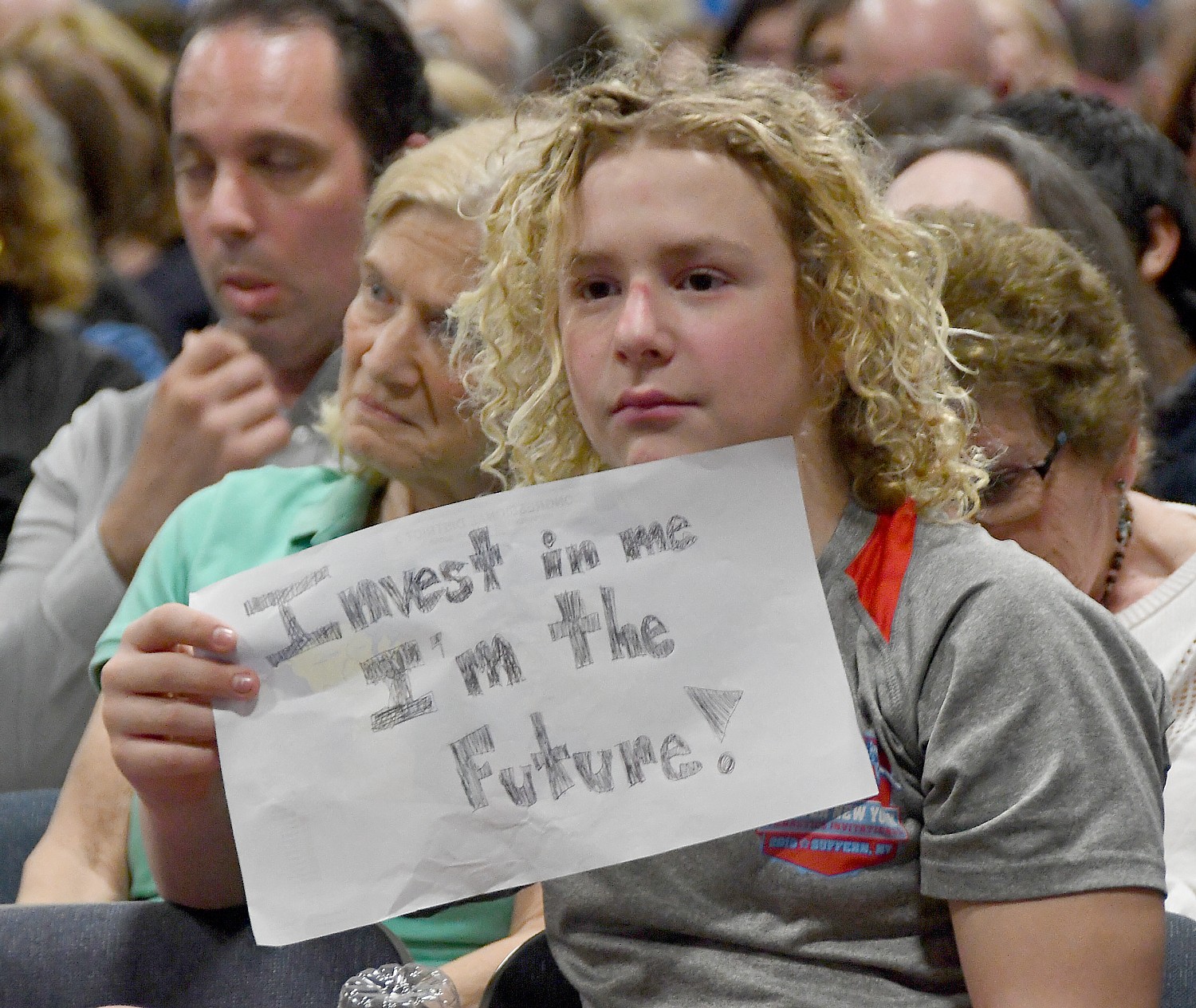
Whenever someone introduced themselves as an expert – such as the scientist with Feinstein Institute who is a member of a newly formed Science Advocacy of Long Island (who have much to be concerned with as the Trump Administration destroys data on climate change and looks to shut down NASA’s Climate monitoring activities) – he would recruit them onto the committee. The high school fellow too young to vote whose friends are completely apathetic? You’re recruited. Get your friends engaged.
“Take that energy, that excitement and use it in a constructive forum to win the battle,” he said.
With the debate swirling over whether Democrats should be as obstructionist as the Republicans were during Obama’s presidency, Suozzi clearly appreciates that “politics is the art of the possible” (as Hillary Clinton said, much to the consternation of the Bernie Sanders ultra-left progressives who likely were among the 92 million voters who did not come out and vote, handing the reins of power and policy to the exact opposite of Obama/Clinton).
Indeed, Suozzi as Congressman is functioning exactly as he said he would during the campaign: as someone who prefers to find common ground in order to accomplish something.
He told the packed audience that filled the room to capacity that he is a member of a newly formed (can you imagine?) Problem Solvers Caucus, consisting of 20 Republicans and 20 Democrats. They are trying to find some consensus on issues such as infrastructure and tax reform (good luck with that).
Interestingly, when Suozzi asked for a show of hands of people who had never been politically engaged before, an estimates 40% of the room raised hands.
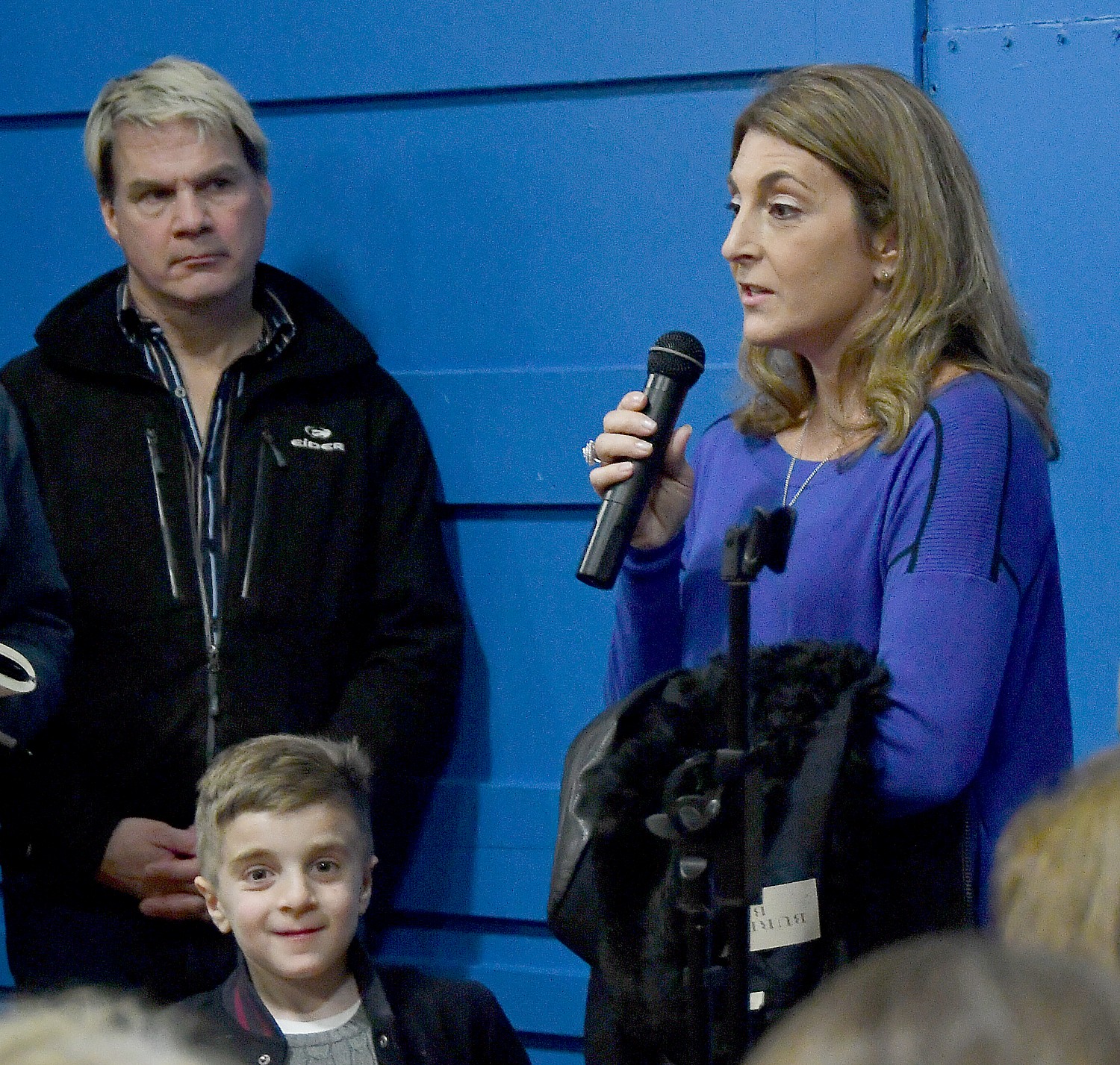
Some of the questions and comments were extremely moving: the woman whose husband is being treated, thanks to Obamacare, for cancer “he’s on the verge of being cured, but if Obamacare is repealed, he would have a preexisting condition”; the son whose father has advanced Parkinsons, who lost his job and if Obamacare is repealed, faces the dilemma of providing quality of life for the father or the family.
A woman speaking haltingly because of her disability, fearful of proposals to cut Medicaid, Medicare and Social Security and instead to send money to states to use as a block grant, a fear echoed by parents and of siblings of disabled people, who declared “I’m tired of people characterizing us as lazy”.
An immigrant man whose college-age son can’t get an internship because of his status; the woman who migrated from India 28 years ago as a 15 year old, who described the “extreme vetting” then, which has only gotten more intense under Obama; and people who asked what can be done to alleviate the anxiety in their communities over sweeps.
Suozzi noted that as Glen Cove Mayor he fought against having local police become defacto ICE agents because of the importance of the community having trust in its government and law enforcement and the value of “community policing”.
He also acknowledged when someone brought up something that he was not aware of – like the problem with a local pre-school that serves special needs children which has to negotiate individually for grants from state and county government, and has seen only a 2% increase in funding over the last six years.
“The Third Will be Heard”
Suozzi did not disguise the surprise at the turnout, noting that in his years as an elected official (Mayor, Nassau County Supervisor) well accustomed to holding town halls, he has never seen anything like this.
He asked what groups were represented: a number were newly formed in response to Trump’s election including several Indivisible groups, who came with pre-printed signs “Agree”, “Disagree” (an effective mechanism to communicate with the Congressman. Others included Reach Out America, Moveon.Org, Science Advocacy of Long Island, Long Island Together, Every Child Matters, Planned Parenthood of Nassau County, 10100, NY Civil Liberties Union, Human Rights Campaign, NOW of Nassau-Suffolk, Code Pink Long Island, Long Island OptOut, Huntington Democrats, among others.
One of reasons Democrats lost is because they didn’t mobilize locally, he said, which is why he hopes to try to keep the energy going, and why he kept going back to the need for the people to get the change they want.
He started off with some of his own comments:
Travel Ban? We are less safe, he said, and putting the ramifications of the Muslim ban and curtailment of immigrants and refugees, he said. “There are 80,000 people worldwide in organized terror groups. There are 65 million refugees, due to climate change, civil war, feminism. This is a nation of immigrants, a nation dedicated to two propositions: all men and women are created equal and entitled to respect and dignity.”
The enhanced sweeps of undocumented immigrants (unfurled in a way that shows the lie of only going after the “bad hombres”) “makes us less safe when communities distrust their local police force. People turn to gangs for protection when they are afraid of law enforcement.”
He was asked about the Stop Arming Terrorists Act that Tulsi Gabbard has proposed. “I have to research further,” he said honestly, adding, “It’s true the US funded Osama bin Ladin against the Russians, and Saddam Hussein, and funded the Syrian regime before, and we are still funding the Saudis who fund terror groups. We did it to have access to oil.
“But, for the first time 50 years we are not dependent on oil from the Mideast. This is an opportunity that is not likely to be seized on by the Trump Administration.”
Had Trump not reversed all the Obama policies that bolstered homegrown, clean renewable energy, the US could have said to these dictators, “We don’t want your land your oil. But we need to move more to clean energy to make this happen.” (Trump, in his speech to the CIA the day after the inauguration, as the Women’s March was going past the White House, said that he thought we would have a second chance at taking Iraq’s oil, because he had been taught that “to the victor belongs the spoils.”)
Obamacare: Mend It Don’t End It
On the first topic, Obamacare, a man said he was walking proof of the problems, because his wife suffers from cancer, and over the past two years, one insurance company after another pulled out, until the hospital where his wife was being treated said they would not treat her because there was no carrier in the exchange. Now, his wife has a pre-existing condition.
Suozzi said, “There are problems with ACA. But we need to mend it, not end it.” He said he supported single-payer (essentially Medicare for All), but that wasn’t possible under Obama, who instead bent over backwards, even picking up on the right-wing Heritage Foundation’s model that preserved for-profit health insurance companies as the intermediary for obtaining health care which had been put into place in Massachusetts under Governor Romney. Obama was unable to get a public option. But even after bending over backwards to accommodate Republicans, not a single one voted in favor of ACA, but instead, spent six years voting 60 times to repeal it, even forcing a government shut down.
People raised concern about the proposal to tax people differently for health care based on age, not income, a scheme to cut $216 billion in spending ; of capping how much employers give to employees for health insurance which then would be taxed as income.
“It’s time to get out the Uzzi and go after Price [the new Secretary of Health & Human Services, whose 2015 bill repealing Obamacare is the most likely model]. Go after Republicans for raising taxes.”
A young man described how his father had advanced Parkinsons and then was laid off and lost his health insurance. Now he has a pre-existing condition. Repealing Obamacare, he said, “would force our family to choose between my father’s well-being and our family’s.”
Suozzi responded, “This is real life, the devastating effect of repealing Obamacare.”
Turning next to the Trump-Putin and conflicts of interest topic, Suozzi said he would support a bill to require Trump to release his taxes, and would support an independent (not just bipartisan) commission to investigate his ties to Russia and possible collusion of his campaign with Russian agents to swing the election.
“This is why you are so important,” he said. “I don’t want you to understate what you are doing. It’s working. We need reasonable Americans to put country ahead of party. Since McCarthy, Republicans have tried to paint Democrats as unpatriotic. This is a generational opportunity to change that dynamic.”
A man noted that none of the 7 countries under Trump’s ban has had anything to do with terrorism in the US since 1975 (on the other hand, terrorist acts were committed by people from Pakistan, Afghanistan and Saudi Arabia and none of these were included in the ban), using the premise of public safety. But 34,000 people are killed each year by gun violence.
“Guns kill, not refugees,” a woman said.
Suozzi said that even when he brought together gun rights advocates with gun control advocates, there was general consensus on the need for universal background checks (instead, the Republicans just overturned Obama’s requirement for mentally ill people receiving services from Social Security to be included in the database). The reason there is no commonsense gun regulation is the same that reasonable health care is blocked: moneyed interests. “It’s always about the money.”
But the focus on Trump’s use of fear and under the guise of “national security” push through anti-democratic policies (such as his threat to “send in the feds” to Chicago and use military precision to round up undocumented immigrants with expedited review so that their cases are not properly adjudicated, his attacks on free press and an independent judiciary and reestablish private prisons) prompted a woman to remark, “Be afraid. The America you know won’t exist in 15 years. Republics disappear. Commitment is important. We should be afraid that America will slip away from us, we must persevere.”
This raised the issue of campaign finance reform and gerrymandering and voter suppression. Suozzi confessed his inability to significantly change any of that, but that it is up to the people to get people out to vote, which is another compelling reason for his neighborhood-based activism. He said his office would be engaged in voter registration campaign.
Rachel Carcalelli of Great Neck Plaza, an environmentalist, noted that Superstorm Sandy cost $75 billion. “We need to rebuild infrastructure in sustainable ways – public transportation, water systems, renewable energy, sanitation.”
Instead, Nassau County will see $6.5 million cut in bus service.
In each case, Suozzi went back to his go-to – that people need to stay active and engaged, to join his neighborhood teams in order to spread the word.
Challenged by a Sanders supporter to reject everything the Republicans propose, Suozzi said, “I’ve been in politics 20 years. I won a lot, lost a few. JFK described himself as an idealist without illusions. I’m not a sucker. I still believe in this country, the power of people. Politics is a noble profession. I will remain an idealist as long as I can, but with eyes wide open.”
A woman noted that many in the audience “are new to politics, to this forum” and might be helped to have more realistic expectations of what Suozzi and the Democratic party, being essentially powerless in the House, can achieve.
Indeed, Suozzi offered a dose of reality to many of the speakers, such as when he was asked to solve the eons old problem of campaign finance reform and gerrymandering. “Nice idea but it’s not realistic for junior member in minority party,” he told one speaker. “All the stuff coming over transom – there’s no free time.” He listed what he is engaged in so far: foreign affairs committee, armed services committee,. “I want to focus on important things in the district- the Northport VA, the North Shore plume (the Navy and Grumman are the responsible parties to clean up a 40-year old site estimated at $500 million to clean up); airport noise in northeastern queens, two major research centers (Cold Spring and the Feinstein Institute), a Coast Guard facility. I decided to make the Problem Solvers Caucus one of my big focuses –if I could get Republicans interested in campaign finance reform and gerrymandering.”
The youngest speaker of the evening, Zachary, about seven years old, stood on a chair to say, “Impeach Trump. He’s messed up. How did we get into this mess?”
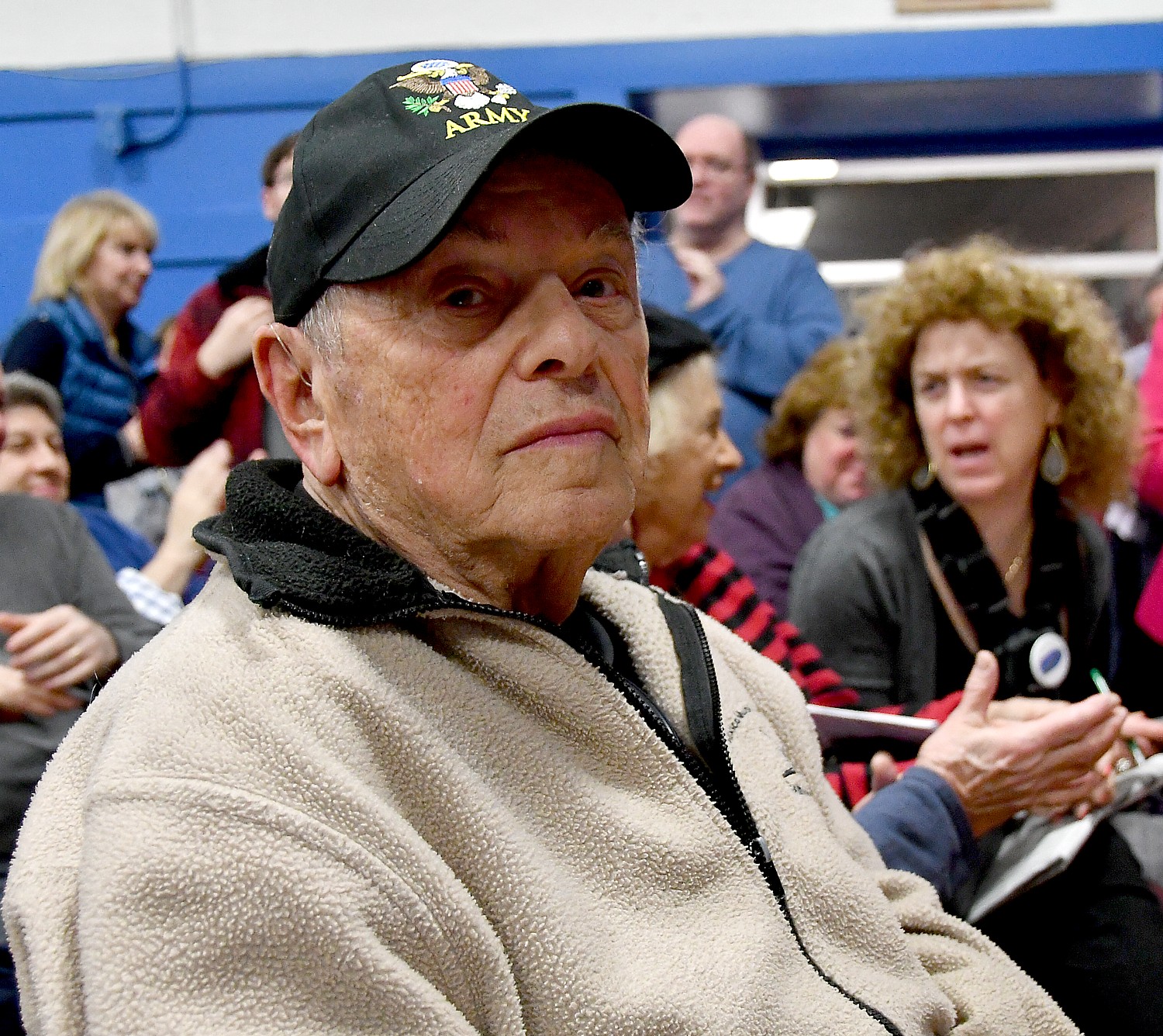
One of the older speakers of the evening, Harry Arlin, wearing an Army baseball cap, said, “I lived briefly under Hitler, had to run; lived under Mussolini and was incarcerated, then under Stalin and had to flee… Now I am living under Trump. Impeach Trump. I’m too old to run again.”
Though the issue of the alarming increase in anti-Semitic incidents across the country since Trump’s election was not specifically raised in this Long Island community with a significant Jewish population, Suozzi acknowledged at one point that the town hall was being held in a Jewish Community Center in Plainview, and JCCs have received over 50 bomb threats in recent weeks.
Suozzi periodically would stop and poll the audience again to get their sense of whether to move on to the next topic. It was remarkable to see how he could actually offer a wide opportunity for people to air grievances, questions, comments in such a large and energized group and have something constructive come out of it: namely, a better understanding of issues and concerns, and also to gauge where constituents are on these key issues.
It wasn’t even close: the 3rd Congressional district wants to retain and improve Obamacare, overturn the travel ban but okay to vet, end the terror and insecurity in immigrant communities and provide a path to some kind of legal status, protect the environment, protect the integrity of the election from foreign influence while protecting the ability of people to cast their ballot.
Gabby Giffords Mocks Republicans Dodging Town Halls
Suozzi’s town hall was very different from what many Republican Congressmen are experiencing around the country – Long Island’s Peter King didn’t even hold one during this President’s Week when traditionally Congress members return to their districts to hear from constituents. Trump and his sycophants have accused those coming out in force to protest the repeal of Obamacare as “paid liberal activists” or, as Trump told CPAC, “the losing side” (neglecting to mention there were 65 million voters, three million more than his side).
And ironically, many of the Republicans are citing fear of their constituents as the reason, prompting Gabby Giffords, who was a Congresswoman until she was shot in the head while holding a public availability at a shopping center in Tucson, to write:
“As a member of Congress, I believed that listening to my constituents was the most basic and core tenet of the job I was hired to do. So I was a little surprised yesterday to hear Congressman Louie Gohmert invoke my shooting as a reason not to face his constituents at a public town hall.
“I was shot on a Saturday morning. By Monday morning my offices were open to the public. Ron Barber – at my side that Saturday, who was shot multiple times, then elected to Congress in my stead – held town halls. It’s what the people deserve in a representative.
“So to Congressman Gohmert and others who are abandoning their civic obligations, I say this: Have a little courage. Face your constituents. Hold town halls.
“Many of the members of Congress who are refusing to hold town halls and listen to their constituents’ concerns are the very same politicians that have opposed commonsense gun violence prevention policies and have allowed the Washington gun lobby to threaten the safety of law enforcement and everyday citizens in our schools, businesses, places of worship, airports, and movie theaters.
“In the past year, campaigning for gun safety, I have held over 50 public events. And if I am still willing to do it, they should be too.”
If Republicans succeed in repealing the Patient Protection and Affordable Care Act (Obamacare), an estimated 2.7 million New Yorkers would lose health coverage, New Yorkers would lose $250 million in Health Care Savings Tax Credits, and New York State would experience a direct state budget impact of $3.7 billion and a loss of nearly $600 million of federal funding that goes directly to counties, which they use to help lower property taxes.
“The cost of a repeal of the Affordable Care Act, to state and local budgets and to the New Yorkers who depend on its health care coverage, is simply too high to justify,” Governor Andrew M. Cuomo said. “Since its implementation, the Affordable Care Act has become a powerful tool to lower the cost of health insurance for local governments and New Yorkers, and it is essential that the federal government does not jeopardize the health and livelihoods of millions of working families.”
The NY State of Health exchange has successfully cut the percentage of uninsured New Yorkers in half, from 10 percent to 5 percent. It has also significantly expanded eligibility and access to health coverage, allowing hundreds of thousands of previously uninsured New Yorkers to achieve economic and healthcare security.
Based on current enrollment levels, the repeal of the Affordable Care Act would result in over 2.7 million New Yorkers losing health coverage. The estimated number of individuals at risk of losing coverage, based on current enrollment levels, is broken down by counties below:
County
Individuals at Risk of Losing Coverage
Albany
25,552
Allegany
4,608
Bronx
300,012
Broome
20,231
Cattaraugus
8,310
Cayuga
7,665
Chautauqua
15,270
Chemung
9,160
Chenango
5,184
Clinton
7,787
Columbia
6,827
Cortland
4,606
Delaware
4,461
Dutchess
25,074
Erie
93,403
Essex
3,660
Franklin
5,110
Fulton
6,038
Genesee
5,074
Greene
4,971
Hamilton
522
Herkimer
6,932
Jefferson
10,955
Kings
540,320
Lewis
2,932
Livingston
4,972
Madison
5,861
Monroe
75,512
Montgomery
5,473
Nassau
133,324
New York
218,937
Niagara
21,287
Oneida
24,781
Onondaga
45,682
Ontario
9,355
Orange
37,851
Orleans
4,522
Oswego
12,568
Otsego
5,785
Putnam
7,006
Queens
493,058
Rensselaer
12,540
Richmond
56,882
Rockland
38,526
Saratoga
16,340
Schenectady
16,056
Schoharie
3,079
Schuyler
2,065
Seneca
3,145
St. Lawrence
11,063
Steuben
10,039
Suffolk
152,631
Sullivan
9,668
Tioga
4,560
Tompkins
7,827
Ulster
19,850
Warren
6,796
Washington
6,689
Wayne
9,354
Westchester
91,844
Wyoming
3,700
Yates
2,515
Total
2,715,807
The estimated direct state budget impact of the repeal is $3.7 billion. New York’s counties have been able to use the additional federal Medicaid funding through the Affordable Care Act, which goes to directly to counties and helps to lower property taxes. A repeal of the Affordable Care Act would result in a total loss of $595 million in funding. A county by county breakdown of the allocated annual funding that each county would lose is available below, based on the most recent year:
County
2016-17 Funding
Albany
$4,738,862
Allegany
$786,300
Broome
$3,049,122
Cattaraugus
$1,211,333
Cayuga
$1,098,606
Chautauqua
$2,443,709
Chemung
$1,491,573
Chenango
$686,373
Clinton
$1,292,531
Columbia
$833,957
Cortland
$786,023
Delaware
$666,830
Dutchess
$2,974,044
Erie
$17,149,148
Essex
$400,176
Franklin
$681,442
Fulton
$879,897
Genesee
$691,774
Greene
$832,298
Hamilton
$68,800
Herkimer
$956,261
Jefferson
$1,601,068
Lewis
$294,378
Livingston
$686,242
Madison
$842,891
Monroe
$13,023,431
Montgomery
$797,695
Nassau
$17,866,829
Niagara
$3,849,704
Oneida
$4,169,425
Onondaga
$7,871,592
Ontario
$1,042,122
Orange
$5,021,173
Orleans
$667,917
Oswego
$2,281,144
Otsego
$729,112
Putnam
$561,094
Rensselaer
$2,307,076
Rockland
$3,867,080
St. Lawrence
$1,564,073
Saratoga
$1,864,638
Schenectady
$2,462,377
Schoharie
$475,760
Schuyler
$312,126
Seneca
$369,493
Steuben
$1,514,370
Suffolk
$18,310,813
Sullivan
$1,439,822
Tioga
$589,433
Tompkins
$1,015,126
Ulster
$2,935,566
Warren
$787,632
Washington
$746,252
Wayne
$910,595
Westchester
$15,243,258
Wyoming
$382,781
Yates
$282,426
Upstate Total
$162,405,572
New York City Total
$433,294,428
New York State Total
$595,700,000
“New York’s healthcare workers see the positive impact of the Affordable Care Act every day,” George Gresham, President, 1199SEIU United Healthcare Workers East, said. “Our patients are able to access preventative care instead of coming to emergency rooms in states of advanced illness. Our employers have reduced losses from uncompensated care. Our friends and relatives are relieved of the fear that getting sick equals financial ruin. Repealing the Affordable Care Act without an adequate replacement would have immediate and devastating consequences for millions of our fellow New Yorkers and for state and local budgets. We applaud Governor Cuomo’s leadership in educating New Yorkers about costs and are proud to stand with him to advocate for the health all New Yorkers,”
Greater New York Hospital Association President Kenneth E. Raske said,“These deeply troubling numbers are only the tip of the iceberg if the Affordable Care Act is repealed. It will also severely harm the hospital community. 27 hospitals across New York State are on a ‘watch list’ for financial stress and many more both public and private face similar fiscal challenges. Repealing the Affordable Care Act without an immediate and adequate replacement plan will make things dramatically worse for safety net hospitals and the vulnerable communities they serve. I applaud Governor Cuomo for his leadership and look forward to working with the bipartisan members of the New York Congressional delegation to ensure that the health care of all New Yorkers is protected.”
“In addition to providing care to those in need, hospitals are major employers in communities all across the state,” stated Bea Grause, President of the Healthcare Association of New York. “Repeal of the ACA could have tremendous consequences for the delivery of healthcare and also in terms of jobs and economic activity. It’s imperative that Congress be mindful of this reality. I’m pleased to join the Governor in this important effort to protect New Yorkers.”
“For too long, Americans paid for health insurance that did not recognize that treatment for mental health and substance use disorders is as essential as other medical treatment,” the White House stated in a Fact Sheet describing steps the Federal Parity Task Force is taking to strengthen indusrance coverage for mental health and substance use disorders. “Untreated mental health and substance use disorders can be debilitating and life-threatening. These consequences are apparent in the prescription opioid and heroin epidemic, as well as the troubling rates of suicide and severe mental illness in this country.
“One of the many important provisions of the Affordable Care Act and the Mental Health Parity and Addiction Equity Act is to ensure that health insurance plans treat mental health and substance use disorders the same way that they treat other health conditions. In March of this year, President Obamaestablishedthe Mental Health and Substance Use Disorder Parity Task Force and charged Federal Departments and Agencies to work together to ensure that Americans are benefiting from the mental health and substance use disorder parity protections under the law. Parity aims to eliminate restrictions on mental health and substance use coverage – like annual visit limits, higher copayments, or different rules on how care is managed such as frequent pre-authorization requirements or medical necessity reviews – if comparable restrictions are not placed on medical and surgical benefits.”
In itsfinal report, the Task Force announced a series of actions and recommendations to help ensure better implementation of parity; to help consumers, providers, and plans understand how parity works; and to ensure appropriate oversight and enforcement of parity protections.
These steps are based on input the Task Force received through a series of listening sessions between March and October held with consumers, providers, employers, health plans, and State regulators, and through the more than 1,100 public comments the Task Force received from individuals with mental health and substance use disorders, families, their providers, advocates, and other stakeholders.
“These recommendations are subject to future budget and policy deliberation,” The White House noted. “Together, today’s steps build on the ongoing work of the Administration to make the treatment of mental health and substance use disorders a priority. The Affordable Care Act ended insurance discrimination based on pre-existing conditions, including mental health and substance use disorders; required coverage of mental health and substance use disorder services in non-grandfathered plans in the individual and small group insurance markets; ensured that recommended preventive screenings, including for depression and alcohol misuse, are available with no co-pays; and expanded Medicaid to millions of additional Americans, significantly improving coverage for mental health care and substance use disorder treatment. In addition, the Administration has issued final regulations providing parity protections to individuals covered through the employer and individual insurance markets, people covered through Medicaid managed care organizations and the Children’s Health Insurance Program, and service members and their families covered through TRICARE.
“Through these steps, the country has made significant progress in expanding mental health and substance use disorder coverage and parity protections for millions of Americans. The Task Force report focuses on parity-related actions and recommendations and does not include the provisions in the President’s Budget that would further expand access to care, including new investments in treatment capacity. The actions and recommendations announced today will continue to advance the Administration’s progress on parity implementation.”
·The Centers for Medicare & Medicaid Services (CMS) is awarding $9.3 million to States to help enforce parity protections. CMS funding will help State insurance regulators work to ensure issuer compliance with the mental health and substance use disorder parity protections.
·The Department of Health and Human Services (HHS), in partnership with the Department of Labor (DOL) and other Task Force agencies, is releasing the beta version of a new parity website to help consumers find the appropriate Federal or State agency to assist with their parity complaints, appeals, and other actions. The Task Force received many comments about the challenges consumers face in identifying the appropriate agency that regulates their insurance coverage. The beta site is being released today for public comment. In the future, the Task Force Departments intend to work together to build out additional functionality on the website related to complaint and data tracking.
·The Substance Abuse and Mental Health Services Administration (SAMHSA) and DOL are releasing aConsumer Guide to Disclosure Rights: Making the Most of Your Mental Health and Substance Use Disorder Benefitsto help consumers, their representatives, and providers understand what type of information to ask for when inquiring about a plan’s compliance with parity and to explain the various Federal disclosure laws that also require disclosure of information related to parity. The Guide includes 11 scenarios, each with specific suggestions for information consumers have a right to that can help, as well as timing requirements for plans and issuers providing these documents.
·DOL is announcing that it will releaseannual data on closed Federal parity investigations and will report on the findings, including the violations citedto ensure parity compliance and inform future policymaking efforts. This effort builds on the 1,515 investigations related to the Mental Health Parity and Addiction Equity Act and 171 violations cited by DOL since October of 2010.
·Toensure parity compliance in plans required to offer essential health benefits, CMS has added Mental Health Parity and Addiction Equity Act compliance to its review of plans subject to the essential health benefits requirement under the Affordable Care Act, and it expects State regulators to do so as well.
·DOL, HHS, and the Department of Treasury (Treasury) are issuingguidance on parity and opioid use disorder treatmentto address specific questions the Departments have received related to issues such as the application of parity to opioid treatment access and coverage of court-ordered treatment.
·HHS, DOL and Treasury aresoliciting feedback on how the disclosure document request process can be improved(input is being sought through the FAQ process), while continuing to ensure consumers’ rights to access all appropriate information and documentation. The request solicits input on the option of developing model forms for parity-related disclosure requests.
·SAMHSA is announcing that it will hosttwo State Policy Academies on Parity Implementation for State Officialsin Fiscal Year 2017, including one focused on the commercial market and one on parity in Medicaid and the Children’s Health Insurance Program. These policy academies will bring together national experts to provide technical assistance to teams of State officials on strategies to advance parity compliance and lessons learned from other States’ implementation efforts.
·CMS will undertake areview of mental health and substance use disorder benefits in Medicare Advantage plansand identify any necessary improvements to advance parity protections.
·DOL, HHS, and Treasury are issuing aParity Compliance Assistance Materials Index. The Departments have issued a total of 44 Frequently Asked Questions (FAQs) over the past six years related to parity, generally as part of larger guidance documents, as well as other parity materials. Several commenters suggested to the Task Force that putting all the parity-related FAQs and guidance together in one place would make the information easier to find and use for States, plans consumers, and other stakeholders.
In addition, the Task Force made the following recommendations:
•Create a one-stop consumer web portal to help consumers navigate parity,which will build out the functionality of the beta parity website released today. The Task Force recommends that the website should help consumers solve coverage issues, file a complaint, or submit an appeal, and also be used to better inform parity oversight and enforcement efforts.
•Increase Federal agencies’ capacity to audit health plans for parity compliance. The Task Force recommends that agencies’ future budgets include funding to expand audit capacity. Given current resources, Federal parity enforcement efforts to date have generally focused on investigating consumer, provider and other parity complaints. Agencies’ capacity to expand enforcement activities, including conducting random audits, is limited by their staffing resources.
•Undertakea detailed review of the non-quantitative treatment limits applicable to substance use disorder benefits in the Federal Employees Health Benefits (FEHB) Program. The Task Force received comments suggesting that non-quantitative treatment limits in FEHB plans may need examination and modification to ensure full compliance, as well as comments suggesting that consistent definitions of terms relating to residential treatment would provide greater transparency for consumers. The U.S. Office of Personnel Management has agreed to conduct this review over the coming year, and take corrective action as indicated by the findings.
•Allow the Department of Labor to assess civil monetary penalties for parity violations. Civil monetary penalty authority would lead to more meaningful penalties for non-compliance with parity. The Task Force recommends that Congress provide the Department of Labor with this authority.
•Develop examples of parity compliance best practices and of potential warning signs of non-compliance. Building on the 2016 DOL/HHS “Warning Signs” document identifying non-quantitative treatment limitations that require additional analysis to determine if they are in compliance with parity, the Task Force recommends a Warning Signs 2.0 document and encourages the inclusion of network adequacy issues in the document. The Task Force also recommends developing further examples of parity compliance best practices to illustrate appropriate application of non-quantitative treatment limitations that are comparable between mental health/substance use disorder benefits and medical/surgical benefits.
•Provide Federal support for State efforts to enforce parity through trainings, resources, and new implementation tools, including model compliance templates. The Task Force recommends continued Federal efforts to provide training and other resources to States to support compliance efforts including partnerships between State mental health/substance use, Medicaid, and State insurance agencies. Further, the Task Force recommends that Federal regulators work with the National Association of Insurance Commissioners and the States to develop a standardized template that States might use to help assess parity compliance. The Task Force also encourages Federal regulators, the National Association of Insurance Commissioners, and other stakeholders to consider a joint effort to develop a model prior authorization form and other model forms.
•Provide simplified disclosure tools to provide consistent information for consumers, plans and issuers. To facilitate disclosure, the Task Force recommends that, in coordination with the National Association of Insurance Commissioners, templates and other sample standardized tools be developed to improve consumer access to plan information.
•Expand consumer education about parity protections. The Task Force recommends continuing and expanding the work to educate consumers about parity and partnering with consumer groups to increase consumer awareness and understanding of parity protections.
•Clarify that health plan disclosure requirements include medical and surgical benefits. The Task Force heard from commenters that it can be challenging to ensure parity compliance when information on medical and surgical benefits is not readily available to allow for comparison to mental health and substance use disorder benefits. Disclosure of the relevant information used to apply coverage limitations to medical and surgical services is currently required for plans covered under the Employee Retirement Income Security Act (ERISA). The Task Force recommends that Congress extend this requirement to non-ERISA plans.
•Implement the Medicaid and Children’s Health Insurance Program (CHIP) parity final rule in a robust manner. The Task Force recommends that implementation include the development of a parity analysis toolkit to help States assess compliance with the final rules on parity for Medicaid managed care organizations and CHIP programs. The toolkit will review key considerations for defining and classifying mental health and substance use disorder benefits (including intermediate and long term supports and services), conducting claims-based analyses for quantitative treatment limits, identifying and analyzing non-quantitative treatment limits, and considerations for Alternative Benefit Plans and CHIP.
•Expand access to mental health and substance use disorder services in TRICARE.The Task Force recommends the Department of Defense’s continued implementation of the TRICARE final rule on mental health and substance use disorders and parity through contract modifications and DOD’s monitoring of access to mental health and substance use disorder care to ensure parity with medical/surgical care.
•Eliminate the lifetime day limit on Medicare Part A treatment in psychiatric hospitals. In Medicare Part A (hospital coverage), there is a 190-day lifetime limit on inpatient treatment in psychiatric hospitals while there is no such limit on inpatient medical/surgical hospital treatment. The Task Force recommends that Congress eliminate the psychiatric hospital lifetime day limit, consistent with the President’s 2017 budget request.
•Update guidance to address the applicability of parity to opioid use disorder services. The Task Force recommends issuing guidance clarifying the application of parity to opioid use disorder treatment benefits in response to specific scenarios associated with these benefits raised by consumers and other stakeholders and updating this guidance regularly, as warranted.
•Eliminate the parity opt-out process for self-funded non-Federal governmental plans. Currently, self-funded non-Federal governmental plans have the ability to elect to not comply with certain Federal provisions including the Mental Health Parity and Addiction Equity Act, which deprives thousands of employees of State and local governments of the mental health and substance use disorder parity protections. The Task Force recommends that Congress eliminate the ability of these plans to opt out of these protections.
Before the Affordable Care Act (ACA, better known as Obamacare), more than 50 million Americans were without any health insurance and 20,000 people were losing their health insurance each month as the Bush Great Recession hemorrhaged 850,000 jobs a month. Though employers for more than a decade have been cutting back on health benefits (making it a Hobson’s choice to leave a terrible job or an abusive marriage), 170 million people get their insurance through their employment, and insurance companies were raising premiums annually at rates five times the rate of inflation, refusing to provide insurance based on pre-existing conditions, charging women higher rates (because they have babies, don’t you know), arbitrarily denying services, capping lifetime claims, throwing people off insurance, and pocketing 25-30% of the premium, with only 70-75% going to patient care.
The Affordable Care Act, designed to make health insurance accessible to everyone, made improvements that have benefited everyone (as Hillary said), but meant the difference between life and death for the 50 million who could not afford health care at all. But to get it passed Obama had to make compromises, including giving up a public option. Then, chiefly Republican-dominated states rejected ACA, casting millions of their residents into a limbo where they could not qualify for the federally-provided exchange and didn’t have access through an employer.
Significantly, ACA (Obamacare) was a Hail Mary to get universal access to health care, with some benefits in terms of containing health care costs. But the next round of health care reform would need to address costs. Here, in the words of their own campaigns, are the candidates’ health plans – in essence, Donald Trump pledges to repeal Obamacare and replace it by returning to “market” (that is, for-profit insurance companies) control, while Hillary Clinton is vowing to make necessary improvements to Obamacare to continue the goal of universal health care, correcting the inequities between states which refused Obamacare and possibly with a public option – Karen Rubin, News & Photo Features.
Trump: Obamacare is a Disaster and Needs to be Repealed
“Obamacare Is A Disaster. You Know It We All Know It.”
During the second presidential debate, the question was asked, “What will you do to bring down the cost of health care? This is the rambling, nonsensical reply to the question, and the Trump campaign is so proud of it, they emailed it out:
TRUMP: “It is such a great question, and it’s maybe the question I get almost more than anything else. Outside of defense. Obamacare is a disaster. You know it we all know it. It is going up at numbers that nobody has ever seen worldwide. No One has ever seen numbers like this for healthcare. It is only getting worse. In seventeen, implodes by itself. Their methods of fixing it is to go and ask Congress for more money. More and more money. We right now have almost twenty trillion dollars in debt. Obama care with mother work. It is very bad, very bad health insurance. Far too expensive, and not only expensive for the person that has it, unbelievably expensive for our country. It’s got to be one of the biggest line items very shortly. We have to repeal it, and replace it with something absolutely much less expensive. And something that works. Where your plan can actually be tailored. We have to get rid of the lines around the state, and official lines. Where we stop insurance companies from coming in and competing because they wanted President Obama and whoever is working on it. They want to leave those lines because that gives the insurance companies, essentially, monopolies. We want competition. You will have the finest healthcare plan there is, she wants to go to a single-payer pan. Which would be a disaster. Somewhat similar to Canada. And if you haven’t noticed the Kitty Indians, when they need a big operations they come into the United States in many cases. Because they are system is so slow, it is catastrophic in certain ways. But she wants to go to single-payer. Which means the government basically rules everything. Hillary Clinton has been after this for years. Obamacare was the first step. Obamacare is a total disaster. And not only are your rates going up by numbers that no one has ever believed, but your deductibles are going up. So that unless you get hit by a truck, you are never going to be able to use it. It is a disastrous plan and it has to be repealed.” (Click To Watch)
Clinton’s Plan To Improve Our Health Care And Build On The Affordable Care Act
“Hillary Clinton will defend and expand on the progress made under Obama Administration toward universal coverage through the Affordable Care Act. The fact is, Hillary has never given up on the fight for universal coverage—and she won’t stop now. As First Lady, she refused to give up when the insurance industry and special interests attacked her and defeated healthcare reform. Instead, she worked with Republicans and Democrats to help create and implement the Children’s Health Insurance Program, which now provides health coverage to more than 8 million children,” Hillary for America campaign stated.
As president, Hillary will build on the Affordable Care Act to expand coverage for millions of Americans.
She will lower-out-of-pocket expenses for consumers purchasing health insurance on the Obamacare exchanges. Hillary believes that in order to expand coverage for families, we need to reduce the cost of purchasing health insurance on the Affordable Care Act exchanges. Her plan will provide enhanced relief for people on the exchanges, and provide a tax credit of up to $5,000 per family to offset a portion of excessive out-of-pocket and premium costs above 5% of their income. She will enhance the premium tax credits now available through the exchanges so that those now eligible will pay less of a percentage of their income than under current law and ensure that all families purchasing on the exchange will not spend more than 8.5 percent of their income for premiums. Finally, she will fix the “family glitch” so that families can access coverage when their employer’s family plan premium is too expensive.
She will support new incentives to encourage all states to expand Medicaid. Hillary will fight for health insurance for our lowest income residents living in every state across the nation. Hillary will follow President Obama’s proposal to allow any state that signs up for the Medicaid expansion to receive a 100 percent match for the first three years, and she will continue to look for other ways to incentivize states to expand Medicaid to meet the health needs of their most vulnerable residents.
She will invest in navigators, advertising and other outreach activities to make enrollment easier. Today, as many as 16 million people or half of all those uninsured are eligible but not enrolled in virtually free Medicaid coverage or exchange coverage for as little as $100 a month or less. Hillary will ensure anyone who wants to enroll can understand their options and do so easily, by dedicating more funding for outreach and enrollment efforts. She will invest $500 million per year in an aggressive enrollment campaign to ensure more people enroll in these extremely affordable options.
She will expand access to affordable health care to families regardless of immigration status. Hillary sponsored the Immigrant Children’s Health Improvement Act in the Senate, which later became law and allows immigrant children and pregnant women to obtain Medicaid and CHIP. She believes we should let families—regardless of immigration status—buy into the Affordable Care Act exchanges. Families who want to purchase health insurance should be able to do so.
She will continue to support a “public option”—and work to build on the Affordable Care Act to make it possible. As she did in her 2008 campaign health plan, and consistently since then, Hillary supports a “public option” to reduce costs and broaden the choices of insurance coverage for every American. To make immediate progress toward that goal, Hillary will work with interested governors, using current flexibility under the Affordable Care Act, to empower states to establish a public option choice.
Going forward, Hillary will build on these efforts and fight to ensure that the savings from these reforms benefits families—not just insurance companies, drug companies, and large corporations. She will expand coverage for Americans living in rural areas and continue a lifelong commitment to protecting women’s reproductive rights.
Hillary’s plan will reduce the cost of prescription drugs. Prescription drug spending accelerated from 2.5 percent in 2013 to 12.6 percent in 2014. It’s no wonder that almost three-quarters of Americans believe prescription drug costs are unreasonable. Hillary believes we need to demand lower drug costs for hardworking families and seniors and she will hold drug companies accountable for unjustified price hikes with new penalties.
Her plan will transform our healthcare system to reward value and quality. Hillary is committed to building on delivery system reforms in the Affordable Care Act that improve value and quality care for Americans.
Hillary will also work to expand access to rural Americans, who often have difficulty finding quality, affordable health care. She will explore cost-effective ways to broaden the scope of health care providers eligible for telehealth reimbursement under Medicare and other programs, including federally qualified health centers and rural health clinics. She will also call for states to support efforts to streamline licensing for telemedicine and examine ways to expand the types of services that qualify for reimbursement.
Hillary is continuing a lifelong fight to ensure women have access to reproductive health care. As senator, she championed access to emergency contraception and voted in favor of strengthening a woman’s right to make her own health decisions. As president, she will continue defending Planned Parenthood, which provides critical health services including breast exams and cancer screenings to 2.7 million patients a year. And she will work to ensure that all women have access to preventive care, affordable contraception, and safe, legal abortion—not just in principle, but in practice, by ending restrictions like the Hyde Amendment.
Hillary for America also challenged Trump’s proposals:
Trump Would Rip Away Health Coverage From 20 Million People And Let Insurers Write The Rules
Donald Trump would immediately work to repeal Obamacare–taking health insurance away from at least 20 million people and letting the insurance companies write the rules all over again. Trump even supported shutting down the government in order to defund Obamacare.
New York Times: “Millions of low-income people have gained coverage under the Affordable Care Act and could lost it if Congress repealed the law.”
Trump saidhe supported Republicans’ efforts to shut down the government over Obamacare and that they should have stuck together.
Trump’s “plan” would cost hundreds of billions more, and does not address people with pre-existing conditions.
CNBC: More $$$, More Uninsured: Donald Trump’s Health-Care Plan
VOX: Trump’s Plan Would Take Health Insurance Away From 21 Million People. Sad!
Bloomberg: “Trump’s proposal is silent on the subject of preventing insurers from dropping coverage for those with preexisting conditions, a feature of Obamacare that Trump has said he supports.”
Meanwhile, the Trump campaign is making hay, taking a statement that President Bill Clinton made out of context:
FACT CHECK: President Clinton And The Affordable Care Act
“Don’t believe Donald Trump when he distorts what President Clinton said about the Affordable Care Act. Bill Clinton, Hillary Clinton, Tim Kaine and President Obama all agree that we have made tremendous progress because of the Affordable Care Act, delivering coverage to 20 million people who were previously uninsured — but they agree there’s more we can do.”
Politifact: “In context, it’s also worth noting that Clinton’s actual comments never mentioned the Affordable Care Act or Obamacare. In fact, as we reviewed the transcript, we noticed that much of what Clinton said addressed issues that pre-dated the 2010 health care law, including concerns about high costs and a lack of guaranteed coverage.”
The bottom line is Hillary will defend and expand on the progress made under Obama Administration toward universal coverage through the Affordable Care Act, while Donald Trump would immediately work to repeal Obamacare, taking health insurance away from 20 million people – and letting the insurance companies write the rules all over again. Trump’s suggested healthcare plan would cost hundreds of billions more, and does not address people with pre-existing conditions.
How much is it worth to you to save your child’s life? $1 million? $10 million? How much is it worth it to you to have the medication that will prolong your mother’s life from Multiple Myeloma, $10,000 a month? (That’s what the medication cost.)
The issue was most recently dramatized by Mylan, the drug company that has a monopolistic control over the EpiPen syringe, and over the course of but a few years, increased the price for an item that can mean the difference between a child surviving a severe allergic response from $57 to $600 (did I mention it has a year-long shelf life?)
The cost of the actual medication, epinephrine, that can stop potentially fatal anaphylactic shock that’s in the EpiPen dispenser? $1.
It’s not just families who are held up, in much the same way as a gun-wielding robber (“Your money or your life”), but school districts, volunteer fire departments and municipalities who can face a severe budgetary crunch.
And it’s not as if Mylan hasn’t already squeezed the profit out of its drug technology – as rapidly as the price has risen, so have the salaries and bonuses paid to its executives.
The steep increase in prices started when drug company Mylan acquired the rights to the EpiPen nearly a decade ago (the company did not even invest in its development). As they hiked the prices, the salaries of their top executives skyrocketed: From 2007 to 2015, Mylan CEO Heather Bresch’s total compensation went from $2.5 million to 3,456 to $18,9 million, a mind-blowing 671% increase.
“I am a for-profit business. I am not hiding from that,” Bresch declared. Indeed, Mylan also dodges paying taxes in America, by using the insidious “inversion” loophole.
In other words, Mylan charges more because it can. Its sole aim is to maximize return for management and investors.
About 40 million Americans have severe allergies to spider bites, bee stings and foods like nuts, eggs and shellfish. Last year, more than 3.6 million U.S. prescriptions for two-packs of EpiPens were filled, earning Mylan nearly $1.7 billion.
What was Mylan’s CEO’s response to the outcry? Mylan said it would expand eligibility for patient assistance, with a $300 savings card.
Mylan is only the latest example. A year ago, the rage was focused on Martin Shkreli, the founder and former chief executive of Turing Pharmaceuticals, who raised the cost of a life-saving drug (which had been available for years from a company he acquired) from an affordable $13.70 a tablet to $750 per tablet.
Another company, Valeant Pharmaceuticals International similarly raised prices of many of its drugs exponentially, including two heart medications, Nitropress and Isuprel used to treat cardiac arrest, and another to treat Wilson’s disease, a rare genetic disorder.
The cynical way they dodge this despicable behavior is to suggest that the consumers don’t actually pay the sticker price – health insurance or Medicare Part D does, or in some cases (as the advertisements like to scream), they offer some relief to the poorest patients. But the upshot is that the rest of us (“society,” if you will) still do pay because of higher premiums. Also, because insurance premiums are so costly, people are opting for cheaper policies that have higher deductibles, so a family might be out-of-pocket to begin with until insurance kicks in.
What is more, the ones who are hurt the most are those who can least afford it: “One of the cruelties of drug pricing is that the burden falls most heavily on those least able to pay it. Uninsured patients often must pay the list price of a drug, and an increasingly large share of insured customers are being asked to pay a percentage of the list price,” writes Katie Thomas in the New York Times. She quotes Pembroke Consulting’s Adam J. Fein, “We soak the poor.”
Not to mention the “donut hole” that many seniors find themselves in. Seniors are finding their costs rising by double digits, 10% in 2015 and 12% in 2014.
There are laws against price-gouging– for food, water, gasoline. There are regulations that keep utility prices – for water, water treatment, electricity – in check, where price hikes have to be justified. Why are there no checks on drug companies, beyond public shaming (which does not seem to work).
The argument is that it costs millions, even a billion dollars and years to research, develop, test and bring a drug to market and many drugs never win approval so never make it to market at all. Well, it also costs millions, even billions, to create a utility system. What is more, taxpayers already pay for a lot of that research, funding programs through universities. (My idea is that taxpayers should be shareholders in the company and get reimbursed through a percentage of the profits on the drug.)
President Obama can use his executive authority to help break Big Pharma’s monopoly power. The FDA controls whether companies can offer alternatives to products like EpiPens, and the National Institutes of Health can prevent new ones from being granted.
Medicare should be allowed to negotiate drug prices (presently inexplicably prohibited under George W. Bush era legislation written by Big Pharma). The Centers for Medicare & Medicaid Services has proposed 6 pilot projects to test possible reforms to how prescription drugs are reimbursed and how the “value” of a drug is measured under Medicare Part B.
Meanwhile, in Congress, Senator Bernie Sanders and Rep. Elijah Cummings of Maryland have introduced bills that would authorize the Secretary of Health and Human Services to negotiate drug prices and reduce barriers to the importation of lower-cost drugs from Canada and other countries.
Another measure being floated in Congress would require a drug company to show justification for any annual price hike greater than 10% (consider that the inflation rate has been running 2%).
But in the absence of Congressional action, California is proposing The California Drug Price Relief Act, which would prohibit the state from paying more for a prescription drug than the lowest price paid for the same drug by Veterans Affairs, which already negotiates lower prices for pharmaceuticals.
“It is no surprise that the pharmaceutical industry already has dedicated $50 million to defeat this ballot initiative,” Sanders said. “Their greed has no end.”
Prices for prescription medicine in the United States soared last year more than 10 percent – the third consecutive year of double digit price increases. One out of five adults between the ages of 18 and 64 – more than 35 million Americans (that’s one out of five)– cannot afford the medications that their doctors prescribe.
Price gouging on life-saving drugs is only one glaring example of why it is an absurdity to operate the health care system as a purely capitalistic, free-market commodity – and yet, this is exactly what is presented by candidates Donald Trump, who vows to repeal Obamacare and the Libertarian Gary Johnson, who thinks that what is wrong with health care system is that there isn’t enough free market forces at work, while Green Party candidate Jill Stein, an actual doctor, has said that the science on childhood vaccinations isn’t definitive.
Hillary Clinton actually has a detailed policy prescription:
Clinton would convene representatives of Federal agencies charged with ensuring health and safety and fair competition, and create a dedicated group charged with protecting consumers from outlier price increases. They will determine an unjustified, outlier price increase based on specific criteria including: 1) the trajectory of the price increase; 2) the cost of production; and 3) the relative value to patients, among other factors that give rise to threatening public health.
Should an excessive, outlier price increase be determined for a long-standing treatment, Clinton’s plan would make new enforcement tools available including:
Making alternatives available and increasing competition: Directly intervening to make treatments available, and supporting alternative manufacturers that enter the market and increase competition, to bring down prices and spur innovation in new treatments.
Emergency importation of safe treatments: Broadening access to safe, high-quality alternatives through emergency importation from developed countries with strong safety standards.
Penalties for unjustified price increase to hold drug companies accountable and fund expanded access: Holding drug makers accountable for unjustified price increases with new penalties, such as fines – and using the funds or savings to expand access and competition.
As it is the system is designed to impede research and development into new drug treatments for ailments and diseases that would not have a big enough pay-back (for example, rarer diseases).
The Obama Administration has supported an initiative which focuses on precision medicine – that is, matching appropriate treatments to genetic make up (it’s why certain asthma treatments are less effective for African-Americans and Hispanics than Caucasians), and how certain cancer treatments (such as envisioned in Biden’s Cancer Moonshot) can be much more targeted.
The Health Care Industrial Complex, however, is not designed to prevent or cure, but prolong the stream of profits.
Hillary Clinton has announced a new plan to protect Americans from unjustified price hikes of long-available prescription drugs with limited competition, like EpiPens and pyrimethamine, the drug for a disease related to AIDS that Turing Pharmaceuticals raised the price of by more than 5,000%. After speaking out against excessive prices for prescription drugs throughout the campaign and, last week, calling for Mylan to lower its EpiPen price, Clinton believes that Mylan’s recent actions have not gone far enough to remedy their outrageous price increase. So today, Clinton is proposing a new set of strong tools – including a consumer protection group – that will let the government take effective action in such cases where public health is put at risk by an unjustified, outlier price increase for a treatment long available on the market with limited competition.
“Over the past year, we’ve seen far too many examples of drug companies raising prices excessively for long-standing, life-saving treatments with little or no new innovation or R&D,” Clinton said. “It’s time to move beyond talking about these price hikes and start acting to address them. All Americans deserve full access to the medications they need — without being burdened by excessive, unjustified costs. Our pharmaceutical and biotech industries are an incredible source of American innovation and revolutionary treatments for debilitating diseases. But I’m ready to hold drug companies accountable when they try to put profits ahead of patients, instead of back into research and innovation.”
Today, building off the comprehensive plan she offered earlier in the campaign last year, Clinton is calling for action to protect consumers from unjustified prescription drug price increases by companies that are marketing long-standing, life-saving treatments and face little or no competition. She’ll start by convening representatives of Federal agencies charged with ensuring health and safety, as well as fair competition, to create a dedicated group charged with protecting consumers from outlier price increases. They will determine an unjustified, outlier price increase based on specific criteria including: 1) the trajectory of the price increase; 2) the cost of production; and 3) the relative value to patients,among other factors that give rise to threatening public health.
Should an excessive, outlier price increase be determined for a long-standing treatment, Clinton’s plan would make new enforcement tools available including:
Making alternatives available and increasing competition: Directly intervening to make treatments available, and supporting alternative manufacturers that enter the market and increase competition, to bring down prices and spur innovation in new treatments.
Emergency importation of safe treatments: Broadening access to safe, high-quality alternatives through emergency importation from developed countries with strong safety standards.
Penalties for unjustified price increase to hold drug companies accountable and fund expanded access:Holding drug makers accountable for unjustified price increases with new penalties, such as fines – and using the funds or savings to expand access and competition.
Her plan will establish dedicated consumer oversight at our public health and competition agencies. They will determine an unjustified, outlier price increase based on specific criteria including: 1) the trajectory of the price increase; 2) the cost of production; and 3) the relative value to patients, among other factors that give rise to threatening public health.
In combination with her broader plan – which addresses the costs facing consumers from both long-standing and patented drugs – these new tools to address price spikes for treatments available for many years will lower the burden of prescription drug costs for all Americans.
This plan would impact the many examples we’ve seen over the past year of drug companies raising prices excessively for drugs that have been available for years – from Turing raising the price of pyrimethamine for AIDS patients by over 5,500 percent, to Mylan raising the price of the EpiPen by more than 400 percent. This is not an isolated problem: Between 2008 and 2015, drug makers increased the prices of almost 400 generic drugs by over 1,000 percent. Many of these companies are an example of a troubling trend—manufacturers that do not even develop the drug themselves, but acquire it and raise the price.
The immediate protections she is offering today build on her broader plan to lower prescription drug costs for all Americans that she released last year.
This week, Hillary Clinton announced her comprehensive plan to support Americans living with mental health problems and illnesses. Recognizing that nearly a fifth of all adults in the United States — more than 40 million people — are coping with a mental health problem, Hillary’s plan will integrate the mental and physical health care systems. Her goal is that within her time in office, Americans will no longer separate mental health from physical health when it comes to access to care or quality of treatment. Hillary has been talking about mental health policy throughout her campaign, since hearing directly from American parents, students, veterans, nurses, and police officers about how these challenges keep them up at night.
According to a Fact Sheet provided by the Hillary for America campaign, Hillary will convene a White House Conference on Mental Health during her first year as President. In addition, her comprehensive agenda on mental health will:
Integrate our nation’s mental and physical health care systems so that health care delivery focuses on the “whole person,” and significantly enhance community-based treatment opportunities. Hillary’s plan will foster integration between the medical and behavioral health care systems (including mental health and addiction services), so that high-quality treatment for behavioral health is widely available in general health care settings. Hillary will expand reimbursement structures in Medicare and Medicaid for collaborative care by tasking the Center for Medicare and Medicaid Innovation to create and implement new such payment models.
Promote early diagnosis and intervention, including launching a national initiative for suicide prevention. The overall rate of suicide increased by 24 percent between 1999 and 2014, and is now at its highest level in 30 years. Hillary will direct all relevant federal agencies, including Health and Human Services, Veterans Affairs, and the Department of Education, to research and develop plans for suicide prevention in their respective settings, and create a cross-government initiative headed by the Surgeon General to coordinate these efforts. She also believes we must redouble our efforts around early screening and intervention – and that means training pediatricians, teachers, school counselors, and other service providers throughout the public health system, to identify mental health problems at an early age and recommend appropriate support.
Enforce mental health parity to the full extent of the law.The Mental Health Parity and Addiction Equity Act of 2008, which Hillary co-sponsored, requires that mental health benefits under group health plans be equal to benefits for other medical conditions, and the Affordable Care Act requires insurance plans in the individual and small group markets to offer mental health coverage as an essential health benefit. But while the right laws are on the books, they are too often ignored or not enforced. As part of her commitment to fully enforcing the mental health parity law, Hillary will launch randomized audits to detect parity violations, and increase federal enforcement. She will also enforce disclosure requirements so that insurers cannot conceal their practices for denying mental health care and strengthen federal monitoring of health insurer compliance with network adequacy requirements.
Improve criminal justice outcomes by training law enforcement officers in crisis intervention, and prioritizing treatment over jail for low-level offenders. As many as 1 in every 10 police encounters may be with individuals with some type of mental health problem, and our county jails today house more individuals with mental illness than our state and local psychiatric hospitals. She will dedicate new resources to help train law enforcement officers in responding to conflicts involving persons with mental illness, and increase grant funding to support law enforcement partnerships with mental health professionals.She will also increase investments in local programs such as specialized courts, drug courts, and veterans’ treatment courts, which send people to treatment and rehab instead of the criminal justice system, and direct the Attorney General to issue guidance to federal prosecutors, instructing them to prioritize treatment over incarceration for low-level, non-violent offenders. Finally, she will work to strengthen mental health services for incarcerated individuals and ensure continuity of care so that they get the treatment they need, which will improve outcomes for them after they reenter society and will reduce recidivism.
Improve access to housing and job opportunities.As president, Hillary will expand community-based housing opportunities for individuals with mental illness and other disabilities. Hillary will launch a joint initiative between the Departments of Housing and Urban Development (HUD) and HHS to create supportive housing opportunitiesfor thousands of people with mental illnesses and disabilities, who currently reside in or are at risk of entering institutional settings. The employment rate for people with serious mental illness is below 20 percent, even though many of these adults want to work and more than half could succeed with appropriate job supports. Hillary will work with private employers and state and local mental health authorities to share best practices around hiring and retaining individuals with mental health problems, and in adopting supported employment programs. She’ll also expand HHS’s “Transforming Lives Through Supported Employment” program, which already assists states and communities in providing supported jobs to people with mental illness.
Invest in brain and behavioral research and developing safe and effective treatments.Hillary believes we need a pioneering, multi-sector effort to transform our knowledge of this field—from mapping the human brain to generating new insights into what drives our behavior to investing in clinical and services research to understand the interventions that work best and how to deliver them to patients. As president, Hillary will significantly increase research into brain and behavioral science research.She will provide new funding for the National Institutes of Health; build on cross-collaborative basic research efforts like the BRAIN initiative; scale up critical investments in clinical, behavioral, and services research; and integrate research portfolios with pioneering work on conditions like PTSD and traumatic brain injury already underway at DoD, the VA, and HHS. She will develop new links with the private and non-profit sectors to ensure that federal government efforts are aligned with those of other sectors to ensure that progress occurs as quickly as possible. She will also commit to brain and behavioral science research based on open data.
The full comprehensive proposal is available on HillaryClinton.com here.
CDC researchers have just concluded that that the virus damages fetal development, resulting in microcephaly and other serious brain anomalies. No other mosquito-borne virus has ever caused birth defects.
That’s just the tip of the iceberg of the public health impacts already being caused by climate change. That’s because changing climate is expanding the habitat for mosquitoes that carry the Zika Virus, Lyme disease and other issues.
Developed over three years by 100 experts in climate-change science and public health – including representatives from the Environmental Protection Agency (EPA), the Department of Health and Human Services (HHS), the National Oceanic and Atmospheric Administration (NOAA), the National Aeronautics and Space Administration (NASA), the Department of Agriculture (USDA), and U.S. Geological Survey (USGS), the Department of Defense (DOD), and the Department of Veteran’s Affairs (VA) – the Climate and Health Assessment reinforces that climate change is a significant threat to the health of Americans not just in the future but right now. As the climate continues to change, the risks to human health will grow, exacerbating existing health threats and creating new public health challenges, and impacting more people in more places. From children to the elderly to pregnant women and the disabled, every American is vulnerable to the health impacts associated with climate change, now and in the future. A few examples of the increased health risks found in the assessment include:
Air pollution and airborne allergens will likely increase, worsening allergy and asthma conditions. Future ozone-related human health impacts attributable to climate change are projected to lead to hundreds to thousands of premature deaths, hospital admissions, and cases of acute respiratory illnesses each year in the United States by 2030, including increases in asthma episodes and other adverse respiratory effects in children. Ragweed pollen season is longer now in central North America, having increased by as much as 11 to 27 days between 1995 and 2011, which impacts some of the nearly 6.8 million children in the United States affected by asthma and susceptible to allergens due to their immature respiratory and immune systems.
Extreme heat can be expected to cause an increase in the number of premature deaths, from thousands to tens of thousands, each summer, which will outpace projected decreases in deaths from extreme cold. One model projected an increase, from a 1990 baseline for more than 200 American cities, of more than an additional 11,000 deaths during the summer in 2030 and more than an additional 27,000 deaths during the summer in 2100.
Warmer winter and spring temperatures are projected to lead to earlier annual onset of Lyme disease cases in the eastern United States and a generally northward expansion of ticks capable of carrying the bacteria that cause Lyme disease. Between 2001 and 2014, both the distribution and the number of reported cases of Lyme disease increased in the Northeast and Upper Midwest.
Increase the risks of water-related illnesses. Runoff from more frequent and intense extreme precipitation events, and increased water temperatures, will increasingly compromise recreational waters, shellfish harvesting waters, and sources of drinking water, increasing risks of waterborne illness.
Climate change, including rising temperatures and changes in weather extremes, is expected to increase the exposure of food to certain pathogens and toxins. Rising temperature and increases in flooding, runoff events, and drought will likely lead to increases in the occurrence and transport of pathogens in agricultural environments, which will increase the risk of food contamination and human exposure to pathogens and toxins. This will increase health risks and require greater vigilance in food safety practices and regulation.
Climate change will have the largest health impact on vulnerable populations including those with low incomes, some communities of color, limited English proficiency and immigrant groups, Indigenous peoples, children, pregnant women, older adults, vulnerable occupational groups, persons with disabilities, and persons with preexisting or chronic medical conditions.
Extreme weather and other events related to climate change will impact health by exacerbating underlying medical conditions, increasing exposure to food-borne and waterborne illness risks, and disrupting infrastructure, including power, water, transportation, and communication systems, that are essential to maintaining access to health care and emergency response services and safeguarding human health.
In addition, the Administration has announced a number of actions to respond to the critical challenges and vulnerabilities outlined in the Climate and Health Assessment. These include:
Developing K-12 educational materials on climate change and health.
A Climate-Ready Tribes and Territories Initiative, which will provide awards for tribal and territorial health departments to investigate, prepare for, and adapt to the health effects of climate change.
Designating May 23-27, 2016, as Extreme Heat Week, during which Federal agencies will take a number of actions to work with community planners and public-health officials to enhance community preparedness for extreme heat events.
The findings of the Climate and Health Assessment strengthen and broaden the scientific foundation for future decision making, allowing individuals, communities, organizations, and governments to proactively manage the health risks of climate change. A better understanding of how climate change affects our health, and the health of our children and grandchildren, underscores the need for urgent action to combat the threats climate change poses on American citizens and communities.
Already, under President Obama’s leadership, the United States has done more to combat climate change and protect the health of communities than ever before. For example, the Clean Power Plan will deliver better air quality, improved public health, clean energy investment and jobs across the country. Since the historic global climate agreement was reached at COP21 in Paris last year (signed on Earth Day at the United Nations), the United States has announced plans to not only implement the agreement to reduce greenhouse gas emissions, but has also committed to adopting an amendment to the Montreal Protocol that would phase down HFCs, a potent greenhouse gas. The Administration has forged a global agreement to cut aviation emissions, and most recently taken a series of actions to reduce methane emissions from the oil and gas sector, while also helping to spur a historic increase in wind and solar energy while doubling the fuel efficiency in our cars.
HOW CLIMATE CHANGE AFFECTS HEALTH:
KEY FINDINGS AND MESSAGES FROM THE ASSESSMENT
Changes in Extreme Heat and Extreme Cold. A warmer future is projected to lead to “on the order of thousands to tens of thousands of additional premature deaths per year across the United States by the end of this century” from heat. Any reduction in cold-related deaths is projected to be smaller than the increase in heat-related deaths in most regions. High temperatures can also lead to a wide range of illnesses. Examples of illnesses associated with extreme heat include cardiovascular, respiratory, and renal illnesses; diabetes; hyperthermia; mental health issues; and preterm births. Even small differences from seasonal average temperatures result in illness and death. An increased risk for respiratory and cardiovascular death is observed in older adults during temperature extremes.
Impacts on Air Quality. Changes in the climate affect the levels and location of outdoor air pollutants such as ground-level ozone and fine particulate matter. These changes in ozone are projected to lead to hundreds to thousands of premature deaths, hospital admissions, and cases of acute respiratory illnesses per year in the United States in 2030. In addition, the area burned by wildfires in North America is expected to increase dramatically over the 21st century due to climate change. Air pollution from wildfires can affect people far downwind from the fire location,increasing the risk of premature death and hospital and emergency department visits. Higher temperatures and increasing carbon dioxide levels also promote the growth of plants that release airborne allergens.
More Frequent and Intense Extreme Events. Climate change will expose more people to increases in the frequency and/or intensity of drought, wildfires, and flooding related to extreme precipitation and hurricanes. Many types of extreme events related to climate change cause disruption of critical infrastructure, including power, water, transportation, and communication systems, that are essential to maintaining access to health care and emergency response services and safeguarding human health. Health risks may also arise long after the event, or in places outside the area where the event took place, particularly if multiple events occur simultaneously or in succession in a given location – this could be the result of damage to property, destruction of assets, loss of infrastructure and public services, social and economic disruption, and environmental degradation. Poverty also is a key risk factor, and the poor are disproportionately affected by extreme events.
Altered Timing and Location of Vector-Borne Disease. Climate change is expected to alter the geographic and seasonal distributions of existing vectors and vector-borne diseases, such as Lyme disease, West Nile virus infections, and other diseases spread by vectors like mosquitoes. Rising temperatures, changing precipitation patterns, and a higher frequency of some extreme weather events associated with climate change will influence the distribution, abundance, and prevalence of infection in the mosquitoes that transmit West Nile virus, the leading cause of mosquito-borne disease in the United States. Outdoor workers are at a greater risk for contracting Lyme disease and, if working in areas where there are infected mosquitoes, occupational exposures can also occur for West Nile virus.
Increased Risks of Water-Related Illnesses. Runoff from more frequent and intense extreme precipitation events will increasingly compromise recreational waters, shellfish harvesting waters, and sources of drinking water, increasing the risk that infrastructure for drinking water, wastewater, and stormwater will fail due to either damage or exceeding system capacity. Although the United States has one of the safest municipal drinking water supplies in the world, water-related outbreaks still occur—between 1948 and 1994, 68 percent of waterborne disease outbreaks in the United States were preceded by extreme precipitation events. Inequities in exposure to contaminated water disproportionately affects tribes and Alaska Natives, residents of low-income rural subdivisions along the U.S.–Mexico border, migrant farm workers, the homeless, and low-income communities not served by public water utilities—some of which are predominately Hispanic or Latino and African-American communities.
Increased Threats to Food Safety and Nutrition. As climate change drives changes in environmental variables, such as ambient temperature, precipitation, and weather extremes (particularly flooding and drought), increases in foodborne illnesses are expected. In the United States, the Centers for Disease Control and Prevention (CDC) estimate that there are 48 million cases of foodborne illnesses per year, with approximately 3,000 deaths. Rising levels of carbon dioxide in the atmosphere can actually lower the nutritional value of most food crops. Climate-change impacts on food production, food processing and utilization, food prices, and agricultural trade were recently addressed in a separate assessment report on Climate Change, Global Food Security, and the U.S. Food System.
Adverse Impacts on Mental Health. The cumulative and interactive effects of climate change, as well as the threat and perception of climate change, adversely impact individual and societal physical and mental health and well-being. Mental health consequences of climate change range from minimal stress and distress symptoms to clinical disorders, such as anxiety, depression, post-traumatic stress, and suicidal thoughts and behaviors. The mental health impacts of extreme events, such as hurricanes, floods, and drought, can be expected to increase as more people experience the stress—and often trauma—of these disasters. People with mental illness and those using medications to treat a variety of mental health conditions such as depression, anxiety, and other mood disorders are particularly vulnerable to extreme weather events and extreme heat.
Disproportionate Effects on Vulnerable Populations. Every American is vulnerable to the health impacts associated with climate change. People at every life stage have varying sensitivity to climate change impacts. The most vulnerable populations include individuals with low income, some communities of color, individuals with limited English proficiency and immigrant groups, Indigenous peoples, children, pregnant women, older adults, vulnerable occupational groups, persons with disabilities, and persons with preexisting or chronic medical conditions.
Communities of Color, Low Income, Immigrants, and Limited-English-Proficiency Groups. Vulnerable populations are at increased risk of exposure given their higher likelihood of living in risk-prone areas (such as urban heat islands, isolated rural areas, or coastal and other flood-prone areas), areas with older or poorly maintained infrastructure, or areas with an increased burden of air pollution. Communities of color, low income, immigrant and limited-English-proficiency groups also experience relatively greater incidence of chronic medical conditions, such as cardiovascular and kidney disease, diabetes, asthma, and chronic obstructive pulmonary disease (COPD), which can be exacerbated by climate-related health impacts.
Indigenous Peoples in the United States. Because of existing vulnerabilities, Indigenous people, especially those who are dependent on the environment for sustenance or who live in geographically isolated or impoverished communities, are likely to experience greater exposure and lower resilience to climate-related health effects.
Pregnant Women. Climate-related exposures may lead to adverse pregnancy and newborn health outcomes, including low birth weight, preterm birth, dehydration and associated renal failure, diarrhea, and respiratory disease. Estimates indicated that there were more than 56,000 pregnant women and nearly 75,000 infants directly affected by Hurricane Katrina and that pregnant women with high hurricane exposure and severe hurricane experiences were at a significantly increased risk for post-traumatic stress disorder (PTSD) and depression.
Children. Climate change—interacting with factors such as economic status, diet, living situation, and stage of development—will increase children’s exposure to health threats. Children are vulnerable to adverse health effects associated with environmental exposures due to factors related to their immature physiology and metabolism, their unique exposure pathways, their biological sensitivities, and limits to their adaptive capacity. Children have a proportionately higher intake of air, food, and water relative to their body weight compared to adults. They also share unique behaviors and interactions with their environment that may increase their exposure to environmental contaminants.
Older Adults. The nation’s older adult population (ages 65 and older) will nearly double in size from 2015 through 2050. Between 1979 and 2004, deaths from heat exposure were reported most commonly among adults aged 65 and older. The need to evacuate an area during or after extreme events can pose increased health and safety risks for older adults, especially those who are poor or reside in nursing or assisted-living facilities. Air pollution can also exacerbate asthma and COPD and can increase the risk of heart attack in older adults, especially those who are also diabetic or obese.
Occupational Groups. Outdoor workers are often among the first to be exposed to the effects of climate change. Climate change is expected to affect the health of outdoor workers through increases in ambient temperature, degraded air quality, extreme weather, vector-borne diseases, industrial exposures, and changes in the built environment. An increased need for complex emergency responses will expose rescue and recovery workers to physical and psychological hazards. The incidence of heat illness among active duty U.S. military personnel is several-fold higher than the summertime incidence in the general U.S. population (147 per 100,000 among the military versus 21.5 per 100,000 in the general population per year)
Persons with Disabilities. An increase in extreme weather can be expected to disproportionately affect populations with disabilities, who experience higher rates of social risk factors—such as poverty and lower educational attainment—that contribute to poorer health outcomes during extreme events or climate-related emergencies. Persons with disabilities often rely on medical equipment (such as portable oxygen) that requires an uninterrupted source of electricity.
Persons with Chronic Medical Conditions. Preexisting medical conditions present risk factors for increased illness and death associated with climate-related stressors, especially exposure to extreme heat. Hospital admissions and emergency room visits increase during heat waves for people with diabetes, cardiovascular diseases, respiratory diseases, and psychiatric illnesses. Medical conditions like Alzheimer’s disease or mental illnesses can impair judgment and behavioral responses in crisis situations, which can place people with those conditions at greater risk.
NEW ADMINISTRATION ACTIONS RESPONDING TO THE
CLIMATE AND HEATH ASSESSMENT
President Obama has already taken action to combat the health impacts of climate change and protect the health of future generations. Just last year, the Administration:
Brought together health and medical professionals, academics, and other interested stakeholders to discuss the challenges of climate change for public health through a series of convenings, workshops, and a formal White House Climate Change and Health Summit;
Expanded access to climate and health data, involving more than 100 health-relevant datasets, to spur innovation so that communities and businesses could act to reduce the health impacts of climate change;
Started integrating climate considerations into agency health and safety policies; and
Created initiatives at EPA, USGS, CDC, and the Department of Defense to improve, consolidate, and better visualize data connecting climate change effects to human health.
The Administration has announced a series of additional actions to keep us on track to better understand, communicate, and reduce the health impacts of climate change on our communities, including:
President’s Task Force on Environmental Health Risks and Safety Risks to Children Addresses Climate Change. The President’s Task Force on Environmental Health Risks and Safety Risks to Children, has expanded its scope to include climate change. The Task Force includes representatives of 17 federal departments and White House offices and focuses on environmental threats to the health and wellbeing of children that are best addressed through interagency efforts. Its priorities are asthma disparities, healthy settings, chemical exposures, and climate change and children’s health. The Task Force has made available examples of actions being taken around the country to protect children from the impacts of climate change on HHS’s new climate and health website at http://www.hhs.gov/climate/childrenshealth/index.html.
Developing a Climate-Ready Tribes and Territories Initiative. This year, CDC’s Climate and Health Program will launch the Climate-Ready Tribes and Territories Initiative, which will provide awards for up to five tribal and territorial health departments in the U.S to support public health preparedness and resilience activities that address the health challenges of climate change in these areas. Although some state and city health departments receive guidance and funding for climate and health research and adaptation planning, no similar program has been available to assist tribal and territorial governments. CDC will work with stakeholders to develop guidance relevant to the unique challenges faced in these jurisdictions. CDC will use its disease prevention expertise to assist tribal and territorial governments in investigating, preparing for, and adapting to the health effects of climate change.
Updating the Sustainable and Climate Resilient Health Care Facilities Toolkit.The Toolkit is undergoing pilot testing and evaluation and will be revised and expanded by the end of the year. In addition, lectures and trainings on the toolkit are being planned for a series of major conferences this year, including the NACCHO Preparedness Summit, the meeting of the American Society for Healthcare Engineering, and the CleanMed Conference. Also planned is a series of training webinars for the private sector on how to use of the toolkit by Practice Greenhealth.
National Institute of Environmental Health Sciences (NIEHS) to Develop K-12 Educational Materials on Climate Change and Health. NIEHS is developing educational materials on climate change and health at the K-12 level based on the new Climate and Health Assessment. They will partner with the National Oceanic and Atmospheric Administration and the American Meteorological Society to help disseminate the materials and offer training. The audience for training is teachers and “train the trainer” teacher experts. The training is expected to be piloted this fall.
Reducing the Health Impacts of Extreme Heat. The Administration is announcing that May 23 – 27 is Extreme Heat Week during which agencies will take a number of activities to prepare the nation for extreme heat. This week is a key part of America’s PrepareAthon!, the Administration’s seasonal campaign to build community-level preparedness action. The White House is planning a webinar during Extreme Heat Week focused on education and outreach to populations more vulnerable to extreme heat as well as to community planners and public health officials to enhance community preparedness to extreme heat events.