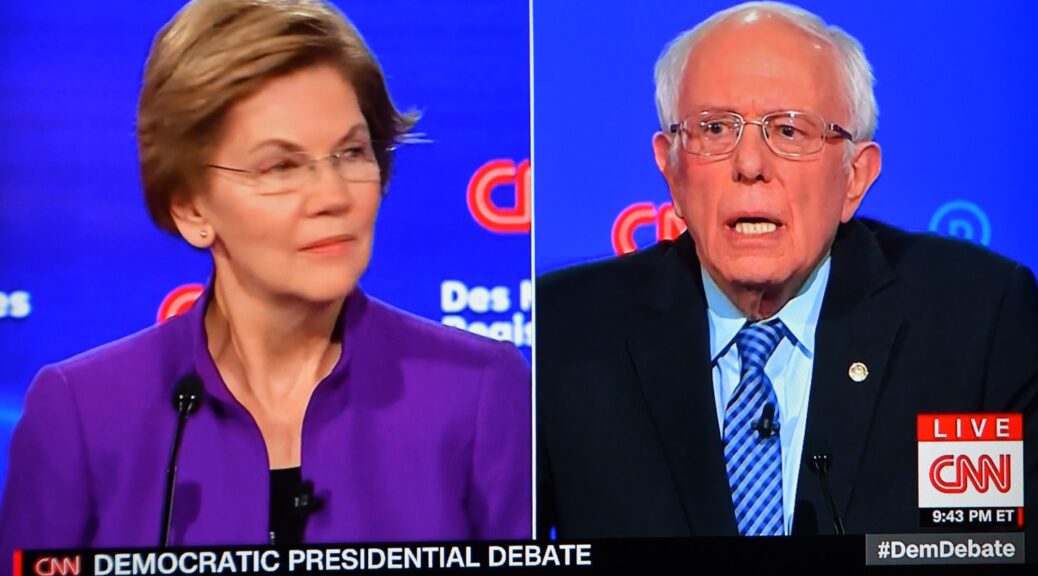
A new study that shows Medicare for All would save Americans $450 billion and 68,000 premature deaths a year could bolster the 2020 presidential campaigns of progressives Senator Elizabeth Warren and Bernie Sanders.
Medicare for All is
ironically, considering that Americans and especially Democrats have indicated
that access to affordable healthcare is their number one priority, is the issue
that could sink the 2020 presidential candidacy of progressives Bernie Sanders and
Elizabeth Warren. Now Sanders is heralding a new study by epidemiologists in
the medical journal The Lancet which found that Medicare for All would save
Americans $450 billion and prevent 68,000 premature deaths a year. Here is
Sanders’ statement:
Sen. Bernie Sanders on Saturday applauded a new study published
today by a team of epidemiologists in the peer-reviewed medical journal The
Lancet, which found that Medicare for All will save Americans $450 billion
and prevent 68,000 unnecessary deaths each and every year.
“This study confirms that Medicare for All will save the American people
$450 billion on health care costs and will prevent 68,000 unnecessary deaths –
each and every year,” Sanders said. “In other words, guaranteeing health care
as a human right by creating a Medicare for All system will cost substantially
less than our current dysfunctional health care system. It will save working
class families thousands of dollars and it will prevent tens of thousands of
Americans from dying each year. While the CEOs in the pharmaceutical and health
insurance industry may not like it, we will end their greed and enact Medicare
for All when I am president.”
According to the study, by replacing premiums, deductibles, co-payments
and out-of-pocket costs with a progressive tax system, Medicare for All will
save the average family thousands of dollars each year and will provide
lower-income households the greatest relief.
Struggling hospitals serving low-income communities would be
particularly helped by Medicare for All by eliminating uncompensated care,
increasing Medicaid reimbursement rates to Medicare levels, and reducing
administrative overhead, according to the study.
The study also debunks several attacks on Medicare for All from the
private health care industry that made well over $100 billion in profits last
year. Doctors and hospitals would see large savings in cost and time from
streamlining our bloated and inefficient administrative and billing system,
allowing doctors to spend more time with patients, the study found.
The study is the latest in a series of studies conducted over the past
three decades that have found that guaranteeing universal health care through a
single-payer health care system would not only dramatically improve the health
and well-being of the American people, it would cost less than our current
dysfunctional health care system that puts profits over people.
Last month, another medical journal found
that 19 out of 22 studies done over the past 30 years concluded that moving to
a Medicare for All, single-payer health care system would cost less than our current
health care system in the first year, and all of the studies showed that it
would cost less within a decade of implementation.
Several of the Democratic candidates for president have demonstrated how they contrast with the current occupant of the Oval Office in terms of how they would lead the country through disasters. Senator Amy Klobuchar released her plan for Global Pandemic Prevention, Detection and Response Policy. This is from Senator Klobuchar’s campaign:
MINNEAPOLIS, MN – The recent outbreak of a new strain of coronavirus is a stark reminder of the persistent threats posed by infectious diseases. Senator Klobuchar believes the United States must continue to lead the global fight to prevent, detect and respond to pandemics. In the Senate, she has championed efforts to address outbreaks at home and abroad. She successfully secured critical funding to combat Ebola in West Africa, helping strengthen health care infrastructure. And as Chair of the Senate Steering and Outreach Committee, she spearheaded efforts to rapidly address the spread of the Zika virus and support local prevention measures and research. As President, she will prioritize taking on global pandemics and protecting U.S. national security. She will:
Renew U.S. leadership and recommit to the Global
Health Security Agenda, an initiative launched under the Obama administration
to respond to the threat that infectious diseases pose to the global community.
Work with our allies and through multilateral organizations
like the World Health Organization to improve local health infrastructure in
at-risk countries and regions.
Fully fund U.S. departments, agencies, and programs
that are on the front lines in preventing and responding to outbreaks, both at
home and overseas, including the Centers for Disease Control and Prevention,
Department of Health and Human Services, National Institutes of Health, State
Department, United States Agency for International Development, Biomedical
Advanced Research and Development Authority, and the President’s Emergency Plan
for AIDS Relief.
Strengthen early-warning systems to detect and
respond to outbreaks on the ground before they spread into full-fledged
pandemics.
Develop the global rapid-response system for
deploying international medical teams to respond to outbreaks at the
source.
Increase stockpiles of existing vaccines and
treatments and streamline delivery systems for rapid deployment during
outbreaks.
Invest in capabilities for accelerating the
production of new vaccines and treatments when new pathogens emerge.
Leverage public-private partnerships that can unlock
new investments and innovations.
The Democratic candidates for president offer stark contrasts to the present occupant of the Oval Office. With a potential coronavirus pandemic creating global anxiety, Senator Elizabeth Warren has just released a detailed plan how she would prevent, contain and treat infectious disease outbreaks at home and abroad.
Charlestown, MA – Senator Elizabeth Warren released her plan to prevent, contain and treat infectious disease outbreaks at home and abroad. Diseases like Ebola virus, Zika virus and most recently, coronavirus demonstrate the real threat that outbreaks pose to our health and security. The United States can be a leader in combating these problems. But to do so, we must invest at home to ensure our public health agencies, hospitals, and health care providers are ready to jump into action when outbreaks strike. And we must invest and partner with other countries to help build strong public health systems abroad.
By properly preparing, we will save lives, strengthen our relationships with allies, protect our interests, and help build resilience to outbreaks and pandemics around the world.
Warren’s Plan to prevent, contain, and treat infectious disease outbreaks will:
Restore White House leadership on health security by designating a senior official to focus solely on this issue and fully funding domestic public health and preparedness at key HHS agencies, in contrast to President Trump’s decision to eliminate this White House role and massive proposed budget cuts to public health;
Restore American leadership in the international community, reversing President Trump’s assault on the State Department and USAID;
Invest in global health security and rejoin global efforts on climate change by changing how diseases emerge and spread, reverse President Trump’s proposed global health cuts and retreat from international climate efforts.
Ensure evidence-based decisions and equity in response to outbreaks, relying on science to contain them and ensuring that all communities get the help they need to stay healthy.
Preventing, Containing, and Treating Infectious Disease Outbreaks at Home and Abroad
In 2014, the world watched as Ebola spread throughout six countries in West Africa and eventually jumped oceans to reach the United States, Spain, Italy, and the U.K. As the outbreak spread, over 50 countries stepped up to help respond. The experience revealed a new global reality: to effectively beat infectious diseases, we need all hands on deck.
In 2015 the state of Indiana experienced an outbreak of HIV stemming from the ongoing opioid epidemic. In a county with a population of less than 25,000, over 200 people contracted the virus. Simultaneously, Zika virus was spreading throughout the U.S. and causing birth defects in children born to some infected pregnant women.
Experts believe the world is due for another bout of pandemic influenza. The latest threat comes from coronavirus, a respiratory condition in the same family of viruses as SARS that is spreading throughout China and just last week reached the United States. With well over 2,000 people infected and a rising death toll, China has restricted the movement of 56 million people. Theworld is watching closely to determine if this will be designated as our next global Public Health Emergency.
Instead of building capacity to combat these problems, Donald Trump has deprioritized global health security and risked putting us on heels in a crisis.
Trump has repeatedly tried to nickel and dime federal programs essential to health security, proposing billions of dollars in cuts so drastic that even leading a House Republican thought they would leave Americans vulnerable. Trump eliminated the key position that coordinates global health security across the many federal agencies that work to keep us safe. And his response to natural disasters that could lead to serious outbreaks, like hurricanes in Puerto Rico, has been basically non-existent.
Like so much else, Trump’s approach to keeping us safe from disease outbreaks is a mess. But when he’s gone, we can fix it.
We can invest at home to ensure our public health agencies, hospitals, and health care providers are ready to jump into action when outbreaks strike. And we can help build strong public health systems abroad. By taking these steps, we will save lives, strengthen our relationships with allies, protect our interests, and help build resilience to outbreaks and pandemics.
That’s why I have a plan to prevent, contain, and treat infectious diseases — one that will help keep America safe and healthy. And as President, I will work across all levels of government here at home and with our many partners abroad to turn that plan into action.
Preventing Transmission and Preparing for Outbreaks The best way to beat a pandemic is to prevent it from starting in the first place. As President, I will work to build the foundations that help us catch infectious diseases before they spread.
Build strong public health systems at home and abroad. Combating infectious diseases requires building health infrastructure that enables us to handle epidemics whenever and wherever they strike. Diseases do not recognize borders — we need a global approach to a global problem. To build strong systems we must:
Fund agencies that prevent and manage outbreaks. President Trump has repeatedly proposed billions in cuts to the agencies responsible for fighting and preventing pandemics, a devastating blow that would put lives at risk. Some of the deepest proposed cuts were to the Centers for Disease Control and Prevention (CDC), which runs essential pandemic prevention and response programs. As President, I will fully fund this work, ensuring that key agencies like the Department of Health and Human Services (HHS), the State Department, and the U.S. Agency for International Development (USAID) have the support they need to do their jobs.
Prepare health departments, health care providers and
hospitals, and other facilities and frontline staff. We must increase
funding for the Public Health Emergency Preparedness (PHEP) cooperative
agreement that supports the critical work of health departments across the
country to prepare for outbreaks, natural disasters, and more. Similarly, we
must continue to support the Hospital Preparedness Program (HPP), which ensures
we equip facilities and train staff on the front lines.
Fully fund the Global Health Security Agenda (GHSA). Designed to build capacity in nearly 50 countries, the GHSA funds work in partnership with other countries to strengthen their public health infrastructure and combat outbreaks before they start. And in a few short years, it is clear that investment has paid off. Under President Trump some of this work has ramped down, but we know that the ability to stop an outbreak requires consistent investment and support. As President, I’ll provide it.
Reduce transmission of infectious diseases at home. By
reducing the transmission of communicable diseases like HIV and Hepatitis C, we
keep families healthy and safe and strengthen our health system’s ability to
respond to global pandemics. That’s why I have a plan to invest $100 billion to
end the opioid epidemic, and why I’ve committed to end the domestic HIV epidemic by
2025 and ensure that patients can afford drugs like PrEP and
Hepatitis C treatments by acting on Day One of my presidency to
lower drug prices.
Move to Medicare for All. When people can’t
access basic health care, infectious diseases are more likely to spread and
cause severe, lasting health effects — as we saw in the recent Indiana HIV outbreak.
This is especially true in underserved communities, who can experience
the effects of outbreaks more
severely. Under Medicare for All, everyone will have high quality health care
they can afford, removing financial barriers for patients who may be contagious
and need to seek care. We all benefit when we stop the spread of infectious
disease faster.
Fully fund critical existing global health work. U.S. investments in global health, including programs that combat HIV and AIDS, tuberculosis, and malaria help build capacity in countries around the world that enables them to better handle epidemics when they strike. As President, I will push to expand funding for the President’s Emergency Plan for AIDS Relief, which funds vital services for individuals living with HIV or AIDS overseas and is a pillar of U.S. global health programs. I’ll also repeal the Trump administration’s heartless Global Gag Rule, which makes organizations that conduct or refer patients for abortion ineligible for global health funds — harming patients and reducing the capacity of other nations’ health systems.
Fight climate change. A changing climate means infectious diseases will spread to new places, and it’s already happening. In 2016, the Zika virus threatened more of the U.S. because changing climates mean the mosquitos that carry it now thrive further and further north. And Lyme disease is expected to increase by 20% in the next decade due to climate change. West Nile is projected to more than double by 2050 due to warming, costing upwards of $1 billion annually. Our health depends on fighting climate change. And I have a lot of plans for that.
Recommit to the Paris Agreement and invest in the Green
Climate Fund. On Day One of my administration, I’ll commit the United
States to rejoin the Paris Agreement, including meeting Obama era commitments
to the Green Climate Fund — a critical funding stream to prevent the spread of
climate fueled pandemics — and backfilling the contribution that the Trump
administration neglected to deliver.
Recognize interconnectedness of human, animal, and environmental health. When it comes to pandemics, we must think about how animal, human, and environmental factors interact. Last year the Trump administration shut down the Predict program to test animals for dangerous pathogens that could cross over to humans. As President, I would restore this essential work. And I will support new scientific research to help understand and predict the impact of warmer temperatures on disease emergence and transmission.
Invest in CDC’s Climate and Health Program. This essential program invests in adaptation for the effects of climate change on our nation’s health, but it’s budget only allows for programs that cover roughly half our population. Rather than follow President Trump’s attempts to kill this program, I will expand it to cover every American so no community is left behind.
Prioritize effective federal management. As President, I’ll take key steps to ensure that the agencies who handle outbreaks have clear leadership, responsibility, and support.
Restore White House leadership position for health
security. President Obama created this position in response to the
Ebola epidemic. In 2018, the Trump administration eliminated it –
and I demanded answers. As
President, I will bring it back, with a formal senior lead in my White House
who focuses solely on global health security and oversees this work across the
entire federal government.
Rebuild the State Department and USAID. American security and health depend on robust diplomacy and development assistance, but the Trump administration has declared war on the State Department and USAID. We must reverse the trend of declining American diplomacy and development aid by creating a 21st century foreign service and corps of development specialists. My plan to rebuild the State Department ensures that we have the diplomats we need leading our engagement with the world to help effectively manage outbreaks.
Build on CDC’s legacy as the world and domestic leader in
public health. The Strategic National Stockpile (SNS) holds our nation’s largest supply of
medical countermeasures and medical supplies. Historically, CDC has managed the
SNS because it has the public health expertise to stock the right medical
countermeasures and ensure they get to communities who need them during an
emergency. In 2018, the Trump administration removed the
SNS from CDC management in an ill-advised attempt to
streamline response activities that could make it easier for drug companies to
lobby for their products to be included. As President, I will move it back to
optimize public health while ensuring coordination with other agencies.
Strengthen the Public Health Emergency Medical
Countermeasures Enterprise (PHEMCE). PHEMCE coordinates the federal
government’s efforts to prepare for potential chemical, biological,
radiological and nuclear threats, as well as from emerging infectious diseases.
We must ensure the PHEMCE fully utilizes expertise from across agencies and
reinvigorate its ability to prepare for and respond to emergencies.
Develop vaccines for infectious diseases. The United States should join it’s peer countries and invest in the Coalition for Epidemic Preparedness Innovations (CEPI), a public/private global alliance focused on vaccine development, and actively participate in global coalitions working toward vaccine development. I have pushed CDC to prepare for pandemic influenza, which must include the development of a universal flu vaccine — a necessity if we want to effectively fight the next strain of pandemic influenza.
Containing Outbreaks and Ensuring Equity Effectively containing infectious diseases requires effective coordination, flexible resources, clear data and communication, and the ability to move fast while not leaving anyone behind.
Ensure surge funding to handle the outbreak. Responding to pandemics costs money. And when it’s needed, it’s needed yesterday. In 2014, Congress did not provide funding to combat Ebola when it was out of control in West Africa, and waited until nearly 3 months after the first case occurred in the U.S. to appropriate additional funding. But epidemics don’t wait for Congress. To have a shot at getting ahead of the next big outbreak, we must appropriate and replenish funding for the Public Health Emergency Fund at HHS. This fund enables HHS to quickly respond to public health crises without waiting for supplemental appropriations from Congress.
Establish the Global Health Security Corps. Sometimes outbreaks occur in places experiencing intense conflict. And when health experts cannot enter those regions, outbreaks can grow exponentially. A bipartisan commission recently proposed creating a global health team that can handle these challenges — doctors, scientists, and aid workers with extensive security training who can go into conflict zones to do contact tracing, build trust in communities experiencing conflict, and work effectively with foreign governments at the local, regional, and national level. As president, I’ll launch this Global Health Security Corps to ensure that we can get the right expertise to the center of an outbreak before it becomes an epidemic.
Mitigate impact on underserved populations. Underserved and disadvantaged populations are hit harder by outbreaks. Adding insult to injury, vulnerable populations are often scapegoated for spreading disease. Outbreak responses must ensure that everyone can get the help they need. This requires constant effort on the front lines – but system-level solutions can help, too.
Practice ethical and evidence-based infection
control. My administration will work with state and local governments
to ensure that disease surveillance and response is based on facts and science,
not fear. We will also reject ill-informed, unscientific, and often
counterproductive travel bans in favor of science-based efforts at isolation
and quarantine. These efforts will be undertaken only when necessary, and we
will provide strict protection of civil liberties for those involved, including
the rejection of any unlawful detentions.
Leverage federal health care programs to respond to disasters.Studies have shown the clear connection between extreme weather events and outbreaks. After Hurricanes Irma and Maria hit the US Virgin Islands and Puerto Rico, for example, fatalities from bacterial Leptospirosis spiked, eventually leading to 26 deaths. In addition, despite the extensive damage to the islands infrastructure, the Trump administration waited months before delivering aid or assistance. I have committed to leveragefederal programs to quickly tailor health care responses to specific environmental disasters or outbreaks in affected communities when they occur.
Build equity protections into preparedness grant funding and government seeded innovations. I will instruct my administration to incorporate equity requirements into health preparedness and response programs to ensure all communities get the resources they need to stay healthy. I have also committed to improve environmental equity mapping via “a rigorous interagency effort to identify cumulative environmental health disparities and climate vulnerabilities and cross-reference that data with other indicators of socioeconomic health.” When the government helps fund development and clinical trials of medical countermeasures, we should be sure to negotiate a fair market price so that everyone can afford it.
Provideaggressive dissemination of reliable information. Communication is an essential element of effectively beating an outbreak. My administration will work with the private sector to promote the distribution of important factual information, to counter misinformation, and to ensure that critical facts are appropriately translated so communities can take the steps needed to stay healthy. The Trump administration banned CDC from using “evidence-based” or “policy-based,” as well as other terms, in official documents–unacceptable for an agency whose mission must be informed by science. In a Warren administration, science will once again be in charge at the CDC.
Uphold principles of open science and transparency. Sharing information about what is happening during an outbreak facilitates problem-solving. We must encourage sharing of specimens and data between researchers and public health officials, urge transparency from foreign governments, and increase support for data sharing platforms. During a public health emergency, publishers should not use paywalls to hide important data or force authors to keep data embargoed until publication. My administration will conduct a full-scale reassessment of the public health informatics supported by the federal government and modernize these systems, building on recent congressional investment. And I have already committed to improve interoperability of electronic health records, which will help providers all across this country see their patients’ medical histories and ensure that more patient data can be securely shared with critical public health databases, while ensuring that patient privacy is maintained.
Effectively partner with foreign governments and multilateral organizations. The U.S. cannot beat outbreaks alone. We must use all our tools, including diplomacy and international collaboration, to work through tough issues and partner with other countries. I’ll lead the world in promoting effective multilateral action, including through Joint United Nations Programme on HIV/AIDS and the Global Fund to Fight AIDS, Tuberculosis, and Malaria. And I’ll bolster our work with the World Health Organization (WHO) to continue reforms started after the 2014 Ebola outbreaks and improve the world’s ability to respond collectively to these crises.
Treating Emerging Infectious Diseases It’s essential that we continue pushing for medical advances — both to treat those who contract diseases and vaccinate against those we can prevent.
Invest in basic science. I have committed to invest $100 billion in the NIH — and $60 billion of that will fund basic science research. And when drug companies break the law, I’ll create a “swear jar” where companies will pay a portion of their profits from publicly-funded research back to the NIH. This funding will expand the research we need to develop vaccines and treatments for infectious diseases we know and novel diseases that have not yet emerged.
Invest and incentivize development of new medical countermeasures. To ensure we are able to effectively surge development during a pandemic, we must build and maintain strong infrastructure for medical countermeasure development. As President, I will ensure that small biotechnology innovators get ongoing support from Biomedical Advanced Research and Development Authority (BARDA), and we will leverage the Food and Drug Administration (FDA’s) expertise in manufacturing and clinical trials to help larger drug manufacturers bring these countermeasures to market at scale.
Bring new treatments to patients. The $40 billion I’ve committed to invest in the NIH will fund the creation of the National Institute for Drug Development — a new institute that will work to bring that basic research of the rest of the NIH into reality for patients. And under Medicare for All, we will be able to better incentivize the private sector development of drugs for which the market is currently broken, like vaccines and antibiotics. Vaccines prevent outbreaks from starting, while antibiotics provide critical protection against infections, and we are in desperate need of new antibiotics to combat resistant infections.
Enable surge support during outbreaks, especially for
diagnostics. BARDA and FDA must be ready to surge at times of
outbreak, when the need to quickly diagnose new cases is essential to
containing an outbreak and properly treating patients. My Administration will
work to provide this support and, when appropriate, use Emergency Use
Authorizations to get new diagnostics into the hands of health care providers
as soon as possible.
Prioritize therapies that work for all populations, especially kids. Therapies are often approved after being tested on populations that are not representative of the patient population. As a result, many therapies in the Strategic National Stockpile are not approved for kids, and some therapies do not work as effectively for racial minorities or women. As President, I will direct the FDA and BARDA to work with drug companies to develop pediatric medical countermeasures and increase the enrollment of underrepresented populations in clinical trials, ensuring that the treatments we develop work well for all of us.
Ensure treatments can reach patients quickly. Time is critical when you’re combating infectious diseases. We must make sure that our system is ready to “turn on” at a moment’s notice. That means we must constantly evaluate our medical countermeasure stockpiles and prepare annual updated biological threat assessments. And during an outbreak, we must quickly distribute medical countermeasures, with proper protections for equitable distribution across communities.
Ensure safety of high security labs. My administration will not allow labs to generate novel viruses with epidemic or pandemic potential, or to perform field testing of such viruses and will closely monitor dual-use research on biological threats and update policies as needed. This knowledge is incredibly important to protect our health, but could be harmful if used as a weapon. And we must be vigilant about lab safety standards and avoid accidentally mailing anthrax or forgetting about smallpox specimens for 50 years.
Diseases like coronavirus remind us why we need robust international institutions, strong investments in public health, and a government that is prepared to jump into action at a moment’s notice. When we prepare and effectively collaborate to address common threats that don’t stop at borders, the international community can stop these diseases in their tracks.
Vice President Joe Biden issued his own criticism of the Trump’s administration’s handling of a potential pandemic, in an op-ed in USA Today: Joe Biden: Trump is worst possible leader to deal with coronavirus outbreak citing the need for the President of the United States to cooperate with international partners to address this pandemic and prevent future ones. Biden writes that this is a moment that requires leadership — leadership that Trump is incapable of delivering — and lays out how his policies will be informed by science and reassert U.S. leadership on global health security.
The Women’s Marches that took place across the country – some 250 of them including Washington DC and New York City – are the opening salvo to the 2020 Election. Make no mistake, this was about voting, realizing that all the issues that they care about hinge on the coming election and not on changing the minds of lawmakers who currently control the levers of power: reproductive freedom and a woman’s right to self-determination; access to the ballot and access to health care; climate action and environmental justice; gun safety and domestic violence; gender equity, sexism and misogyny; discrimination and sexual harassment; immigration reform and human rights. They are all on the ballot this November.
And the Supreme Court and all the courts now
dominated by radical right-wing judges that seek to roll back women’s rights,
civil rights, voting rights, health-care-is-a-human-right. “Ruth Bader
Ginsburg, hold on,” Manhattan Borough President Gale Brewer declared as the
march set off down Columbus Avenue, passed the Trump International Hotel, where
the most animated expressions of outrage against Trump and his administration
were manifest.
A singular, unifying message emerged: Dump Trump and
his henchmen and his enablers.
And a theme for the New York City march organized by Women’s March Alliance (womensmarchalliance.org): Rise & Roar.
The vigorous contest of
Democrats seeking the 2020 presidential nomination has produced excellent
policy proposals to address major issues. Clearly
responding to the backlash against her radical plan to finance Medicare for
All, Senator Elizabeth Warren released details of how she would reduce health
care costs in America, eliminate profiteering from the health care system, and
complete a full transition to Medicare for All in her first term. Warren has
already released her plan to fully finance Medicare
for All when it’s up and running without raising taxes on the middle class by
one penny.
“Medicare for All is
the best way to guarantee health care to all Americans at the lowest cost. I
have a plan to pay for it without
raising taxes on middle class families, and the transition I’ve outlined here
will get us there within my first term as president. Together, along with
additional reforms like my plans to reduce black maternal mortality rates,
ensure rural health care,
protect reproductive rights,
support the Indian Health Service,
take care of our veterans, and
secure LGBTQ+ equality, we will
ensure that no family will ever go broke again from a medical diagnosis – and
that every American gets the excellent health care they deserve. “
This is from the Warren campaign:
On Day One, Elizabeth will use her executive authority
to:
Reverse Donald Trump’s sabotage of Obamacare
Improve the Affordable Care Act, Medicare, and Medicaid.
Protect people with pre-existing conditions
Drastically lower pharmaceutical costs for millions of
families for drugs including Insulin, EpiPens, and drugs that save people from
opioid overdoses.
The first bill Elizabeth will pass is her comprehensive set
of anti-corruption reforms which include ending lobbying as we know it and
knocking back the influence of Big Pharma and insurance companies.
And in her first 100 days, Elizabeth will use a
fast-track legislative process called budget reconciliation to create a true
Medicare for All option that will:
Include all the health care benefits of Medicare for All
described in the Medicare for All Act.
Be immediately free for nearly half of all Americans,
including:
Children under the age of 18
Families making at or below 200% of the federal poverty
level (about $51,000 for a family of four)
Give every American over the age of 50 the choice to enter a
substantially improved Medicare program.
Consumer costs will automatically decline, so eventually
coverage under this plan will be free to everyone
Throughout her first term, she will fight for additional
health system reforms to save money and save lives–including a boost of
$100 billion in guaranteed, mandatory spending for new NIH
research.
And no later than her third year in office, she will pass
legislation to complete the transition to Medicare for All: guaranteed
comprehensive health care for every American, long-term care, vision, dental,
and hearing, with a single payer to reduce costs and produce better health
outcomes.
Elizabeth’s plan can deliver an $11 trillion boost to
families who will never pay another premium, deductible, or co-pay.
And her plan will protect unions and make sure that there’s
support for workers affected by these changes.
My First Term Plan for Reducing Health Care Costs in
America and Transitioning to Medicare for All
I spent my career studying why families went broke. I rang
the alarm bells as the costs for necessities skyrocketed while wages remained
basically flat. And instead of helping, our government has become more tilted
in favor of the wealthy and the well-connected.
The squeeze on America’s families started long before the
election of Donald Trump, and I’m not running for president just to beat him.
I’m running for president to fix what’s broken in our economy and our
democracy. I have serious plans to raise wages for Americans.
And I have serious plans to reduce costs that are crushing our families, costs
like child care, education, housing – and health care.
The Affordable Care Act made massive strides in expanding
access to health insurance coverage, and we must defend Medicaid and the
Affordable Care Act against Republican attempts to rip health coverage away
from people. But it’s time for the next step.
The need is clear. Last year, 37 million American
adults didn’t fill a prescription because of costs. 36 million people
skipped a recommended test, treatment, or follow-up because of costs. 40 million people
didn’t go to a doctor to check out a health problem because of costs. 57 million people
had trouble covering their medical bills. An average family of four with
employer-sponsored insurance spent $12,378 on
employee premium contributions and out-of-pocket costs in 2018. And 87 million Americans
are either uninsured or underinsured.
Meanwhile, America spends about twice as much per
person on health care than the average among our peer countries while
delivering worse health outcomes than many of them. America is home to the best
health care providers in the world, and yet tens of millions of people can’t
get care because of cost, forcing families into impossible decisions. Whether
to sell the house or skip a round of chemo. Whether to cut up pills to save
money or buy groceries for the week. The way we pay for health care in the
United States is broken – and America’s families bear the burden.
We can fix this system. Medicare for All is the best way to
cover every person in America at the lowest possible cost because it eliminates
profiteering from our health care and leverages the power of the federal
government to rein in spending. Medicare for All will finally ensure that
Americans have access to all of the coverage they need – not just what
for-profit insurance companies are willing to cover – including vision, dental,
coverage for mental health and addiction services, physical therapy, and
long-term care for themselves and their loved ones. Medicare for All will mean
that health care is once again between patients and the doctors and nurses they
trust–without an insurance company in the middle to say “no” to access to the
care they need. I have put out a plan to fully
finance Medicare for All when it’s up and running without raising taxes on the
middle class by one penny.
But how do we get there?
Every serious proposal for Medicare for All contemplates
a significant transition period. Today, I’m announcing my plan to expand public
health care coverage, reduce costs, and improve the quality of care for every
family in America. My plan will be completed in my first term. It includes
dramatic actions to lower drug prices, a Medicare for All option available to
everyone that is more generous than any plan proposed by any other presidential
candidate, critical health system reforms to save money and save lives, and a
full transition to Medicare for All.
Here’s what I’ll do in my first 100 days:
I’ll pursue comprehensive anti-corruption reforms to
rein in health insurers and drug companies – reforms that are essential to make
any meaningful health care changes in Washington.
I’ll use the tools of the presidency to start improving
coverage and lowering costs – immediately. I’ll reverse Donald Trump’s
sabotage of health care, protect individuals with pre-existing conditions, take
on the big pharmaceutical companies to lower costs of key drugs for millions of
Americans, and improve the Affordable Care Act, Medicare, and Medicaid.
I will fight to pass fast-track budget reconciliation
legislation to create a true Medicare for All option that’s free for tens of
millions. I won’t hand Mitch McConnell a veto over my health care
agenda. Instead, I’ll give every American over the age of 50 the choice to
enter an improved Medicare program, and I’ll give every person in America the
choice to get coverage through a true Medicare for All option. Coverage under the
new Medicare for All option will be immediately free for children under the age
of 18 and for families making at or below 200% of the federal poverty level
(about $51,000 for a family of four). For all others, the cost will be modest,
and eventually, coverage under this plan will be free for everyone.
By the end of my first 100 days, we will have opened the
door for tens of millions of Americans to get high-quality Medicare for All
coverage at little or no cost. But I won’t stop there. Throughout my
term, I’ll fight for additional health system reforms to save money and save
lives – including a boost of $100 billion in guaranteed, mandatory spending for
new NIH research over the next ten years to radically improve basic
medical science and the development of new medical miracles for patients.
And finally, no later than my third year in office, I
will fight to pass legislation that would complete the transition to full
Medicare for All. By this point, the American people will have
experienced the full benefits of a true Medicare for All option, and they can
see for themselves how that experience stacks up against high-priced care that
requires them to fight tooth-and-nail against their insurance company. Per the
terms of the Medicare for All Act, supplemental private insurance that doesn’t
duplicate the benefits of Medicare for All would still be available. But by
avoiding duplicative insurance and integrating every American into the new
program, the American people would save trillions of dollars on health costs.
I will pursue each of these efforts in consultation with key
stakeholders, including patients, health care professionals, unions,
individuals with private insurance, hospitals, seniors currently on Medicare,
individuals with disabilities and other patients who use Medicaid, Tribal
Nations, and private insurance employees.
And at each step of my plan, millions more Americans will
pay less for health care. Millions more Americans will see the quality of their
current health coverage improve. And millions more Americans will have the
choice to ditch their private insurance and enter a high-quality public plan.
And, at each step, the changes in our health care system will be fully paid for
without raising taxes one penny on middle class families.
Every step in the coming fight to improve American health
care – like every other fight to improve
American health care – will be opposed by those powerful industries who profit
from our broken system.
But I’ll fight my heart out at each step of this process,
for one simple reason: I spent a lifetime learning about families going broke
from the high cost of health care. I’ve seen up close and personal how the
impact of a medical diagnosis can be devastating and how the resulting medical
bills can turn people’s lives upside down. When I’m President of the United
States, I’m going to do everything in my power to make sure that never happens
to another person again.
The First 100 Days of a Warren Administration
Donald Trump has spent nearly every day of his
administration trying to rip health coverage away from tens of millions of
Americans – first by legislation, then by regulation, and now by lawsuit. When
I take office, I will immediately work to reverse the damage he has done.
But I’ll do much more than that.
In my first 100 days, I will pick up every tool Donald
Trump has used to undermine Americans’ health care and do the opposite. While
Republicans tried to use fast-track budget reconciliation legislation to rip
away health insurance from millions of people with just 50 votes in the Senate,
I’ll use that tool in reverse – to improve our existing public insurance
programs, including by giving everyone 50 and older the option to join the
current Medicare program, and to create a true Medicare for All option that’s
free for millions and available to everyone.
But first, we must act to rein in Washington
corruption.
Anti-Corruption Reforms to Rein in Health Industry
Influence.
In Washington, money talks – and nowhere is that more
obvious than when it comes to health care. The health care industry spent $4.7
billion lobbying over the last decade. And health insurance and pharmaceutical
executives have been active in fundraising and donating to
candidates in the 2020 Democratic primary campaign as well.
Today, the principal lobbying groups for the drug companies,
health insurers, and hospitals have teamed up with dozens of other
health industry groups to create the Partnership for America’s Health Care
Future – a front group whose members spent a combined $143 million on
lobbying in 2018 and aims to torpedo
Medicare for All in this election. The Partnership has made clear that “whether
it’s called Medicare for All, Medicare buy-in, or the public option,
one-size-fits-all health care will never allow us to achieve [our]
goals.”
Let’s not kid ourselves: every Democratic plan for
expanding public health care coverage is a challenge to these industries’
bottom lines – and every one of these plans is already being drowned in money
to make sure it never happens. Any candidate who believes more modest reforms
will avoid the wrath of industry is not paying attention.
If the next president has any intention of winning any
health care fight, they must start by reforming Washington. That’s why I’ve
released the biggest set of anti-corruption reforms since Watergate – and why
enacting these reforms is my top priority as president. Here are some of the
ways my plan would rein in the health care industry:
Close the revolving door. My plan will close the revolving door between
health care lobbyists and government, and end the practice of large
pharmaceutical companies like Novartis, United Health, Roche, Pfizer, and
Merck vacuuming up senior
government officials to try and monopolize government expertise, relationships,
and influence during a fight for health care reform.
Tax excessive lobbying. My plan will also
implement an excessive lobbying tax on
companies that spend more than $500,000 per year peddling influence – like
Pfizer, Amgen, Eli Lilly, Novartis, and Johnson & Johnson. Money from the
tax would be used to strengthen congressional support agencies, establish an
office to help the public participate in the rule-making process, and give our
government additional resources to fight back against an avalanche of corporate
lobbying spending.
End lobbyist bribery. My campaign finance plan
will ban all lobbyists – including health insurance and pharma lobbyists – from
trying to buy off politicians by donating or fundraising for their campaigns.
This will shut down the flow of millions of dollars in
contributions.
Limit corporate spending to influence elections. My
plan bans all election-related spending from big corporations with a
significant portion of ownership from foreign entities. That would block major
industry players like UnitedHealth, Anthem, Humana, CVS Health, Pfizer,Amgen, AbbVie, Eli Lilly, Gilead, and Novartis – along
with any trade associations that receive money from them – from spending to
influence elections.
Crowd out corporate contributions with small dollar
donations. I support a constitutional amendment to get big money out
of politics. But until we enact it, my plan would institute a public financing
program that matches every dollar from small donations with six more dollars so
that congressional candidates are answering to the people who need health care
and affordable prescription drugs, rather than health insurance and
pharmaceutical companies.
Passing these reforms will not be easy. But we should enact
as much of this agenda as possible, as quickly as possible. I will also use my
executive authority to begin implementing them wherever possible – including
through prioritizing DOJ and FEC enforcement against the corrupt
influence-peddling game. And I will voluntarily hold my administration to the
standards that I set in my anti-corruption plan so that all our federal
agencies, including those involved in health care, serve only the interests of
the people.
Money slithers through Washington like a snake. Any
candidate that cannot or will not identify this problem, call it out, and
pledge to make fixing it a top priority will not succeed in delivering any
public expansion of health care coverage – or any other major priority.
Immediate Executive Actions to Reduce Costs and Expand
Public Health Coverage.
There are a number of immediate steps a president can take
entirely by herself to lower drug prices, reduce costs, and improve Medicare,
Medicaid, and ACA access and affordability. I intend to take these steps within
my first 100 days.
Dramatically Lower Key Drug Prices
As drug companies benefit from taxpayer-funded R&D and
rake in billions of dollars in
profits, Americans are stuck footing the bill. The average American spends
roughly $1,220 per year on
pharmaceuticals – more than any comparable country. As president, I
will act immediately to lower the cost of prescription drugs, using every
available tool to bring pressure on the big drug companies. I’ll start by
taking immediate advantage of existing legal authorities to lower the cost of
several specific drugs that tens of millions of Americans rely on.
Some drug prices are high because pharmaceutical companies
jack up prices on single-source brand-name drugs, taking advantage of
government-granted patents and exclusivity periods to generate eye-popping
profits. Pharma giant Gilead, for example, launched its
Hepatitis C treatment Harvoni at $94,500-per-twelve week treatment – leaving as many as 85 percent of more than 3 million Americans with
Hepatitis C struggling to afford life-saving treatments.
The government has two
existing tools to combat price-gouging by brand-name drug companies, in
addition to tough antitrust enforcement against companies that abuse our patent
system and use every trick in the book to avoid competition. First, the
government can bypass patents (while providing “reasonable and entire
compensation” to patent holders) using “compulsory licensing authority.” The
Defense Department has used this authority as recently as 2014.
Second, under the march-in provisions of the Bayh-Dole Act, the
government can require re-licensing of certain patents developed with
government involvement when the contractor was not alleviating health or safety
needs. Just in this decade, federal research investments have contributed to
the development of hundreds of drugs –
all of which could be subject to this authority.
But new drugs aren’t the only unaffordable drugs on the
market. Even older, off-patent drugs can be expensive and inaccessible. Lack of
generic competition allows bad actors like Martin Shkreli to
boost the prices of decades-old drugs. Some of the biggest generic drug
companies in the country are now being sued by forty-four states for
price-fixing to keep profits high. Limited competition and other market
failures can also lead to drug shortages. Fortunately, the government can also
act to fix our broken generic drug market by stepping in to publicly
manufacture generic drugs, stopping price gouging in its tracks and bringing
down costs..
On the first day of my presidency, I will use these tools
to drastically lower drug costs for essential medications – drugs with high
costs or limited supply that address critical public health needs. And
during my administration, we will use these tools to make other drugs
affordable as well.
Insulin was discovered nearly 100 years ago as
a treatment for diabetes – but today the drug is still unaffordable for too
many Americans. Eli Lilly’s brand-name insulin prices increased over 1,200% since the 1990s.
Insulin costs are too high because three drug companies –
Novo Nordisk, Sanofi, and Eli Lilly – dominate the market, jacking up prices.
Americans with diabetes are rationing insulin, and
taxpayers are spending billions on it
through Medicare and Medicaid. It’s obscene.
No American should die because they can’t afford a century-old drug that can
be profitably developed for
$72 a year. I will use existing authorities to contract for manufacture of
affordable insulin for all Americans.
EpiPens deliver life-saving doses of
epinephrine, a drug that reverses severe allergic reactions to things like
peanuts and bee stings. Though epinephrine has been around for over a century, the pens
that deliver it are protected by a patent that
limits competition. In 2016, this lack of competition allowed Mylan, EpiPen’s
manufacturer, to jack up EpiPen prices by 400%, leaving
families unable to afford this life-saving medication. Though cheaper versions
have recently entered
the market, prices remain out of reach for
many American families. As president, I will use existing authorities to
produce affordable epinephrine injectors for Americans (and especially
children) who need it.
Naloxone can reverse the effects of an opioid
overdose. In 2017, more than 70,000 people died
from a drug overdose in the United States, with the majority due to opioids.
The opioid epidemic cost Americans nearly $200 billion in
2018, including more than $60 billion in health care costs. Health officials agree that
naloxone is “critical” to curb the epidemic – but easy-to-use naloxone products
like ADAPT Pharma’s Narcan nasal spray and Kaléo’s Evzio auto-injector are
outageously expensive, and the approval of a
generic naloxone nasal spray is tied up in litigation. Kaléo spiked the price of
Evzio by over 550% to “capitalize on the opportunity”
of the opioid crisis, costing taxpayers more than $142 million over
four years. It doesn’t have to be this way: in 2016, it cost Kaléo just 4% of what it
charged to actually make Evzio, and naloxone can be as cheap as five cents a dose.
Both products benefited from government support or
funds in the development of naloxone. My administration will use its compulsory licensing
authority to facilitate production of low-cost naloxone
products so first responders and community members can save lives.
Humira is a drug with anti-inflammatory effects used
to treat diseases like arthritis, psoriasis, and Crohn’s disease. It
is the best-selling prescription
drug in the world, treating millions. AbbVie, Humira’s manufacturer, has doubled the price
of Humira to more than $38,000 a year. In 2017, Medicaid and Medicare spent over
$4.2 billion on it – while AbbVie, its manufacturer, developed a “patent thicket” to
shield itself from biosimilar competition. In May 2019, the company
entered into a legal settlement preventing a competitor from entering the U.S.
market until 2023 – probably because prices went down by up to 80% once
biosimilars entered in Europe. My administration will pursue antitrust action
against AbbVie and other drug companies that pursue blatantly anti-competitive
behavior, and, if necessary, use compulsory licensing authority to facilitate
production, saving taxpayers billions.
Hepatitis C drugs like Harvoni are part of
a class described as
“miracle” drugs. Harvoni’s price tag – $94,500-per-treatment – left 85% of the more than 3 million Americans living
with Hepatitis C without a lifesaving medication, while taxpayers foot a $3.8billion bill. Although
the price has come down in recent years, it is still expensive for
too many. One estimate suggests that by
using compulsory licensing, the federal government could treat all Americans
with Hepatitis C for $4.5 billion – just 2% of the $234 billion it would
otherwise cost. That is exactly what I will do.
Truvada is a drug that – until recently –
was the only FDA-approved form
of pre-exposure prophylaxis, which can reduce the risk of HIV from sexual
activity by up to 99%. Truvada’s
manufacturer, Gilead, relied on $50 million in federal grants to
develop it, but today they rake in multi-billion dollar profits while Americans
struggle to afford it. The CDC estimates a million Americans could benefit from
Truvada, though only a fraction do today – largely due to to its $2,000-a-month price tag, which is nearly thirty times what
it costs in other countries. My administration will facilitate the production
of an affordable version – reducing HIV infections and saving taxpayers billions of dollars each
year.
Antibiotics provide critical protection from
bacterial and fungal infections, and we are in desperate need of new
antibiotics to combat resistant infections. Every year, nearly
three million Americans contract antibiotic-resistant infections – and more
than 35,000 people die. But antibiotics don’t generate much money,
discouraging pharmaceutical investment, causing shortages, and contributing to price hikes.
Earlier this year, one biotech firm filed for bankruptcy after
marketing a new antibiotic, Zemdri, for less than a year. My administration
will identify antibiotics with high prices or limited supply and help produce
them to combat resistance and provide patients with the treatments they need.
Drug shortages leave doctors and patients
scrambling to access the treatments they need, forcing many to ration
medications and use inferior substitutes. Our nation’s hospitals, for example,
are currently experiencing a shortage of
vincristine – an off-patent drug that is the “backbone” of childhood cancer
treatment. The vincristine shortage began when Teva, one of its two suppliers,
made the “business decision” to stop manufacturing the drug. When I am
president, the government will track drugs in consistent shortage, like
vincristine, and I will use our administrative authority to ensure we have
sufficient production.
Finally, I will also direct the government to study whether
other essential medicines, including breakthrough drugs for cancer or high-cost
drugs for rare diseases, might also be subject to these interventions because
they are being sold at prices that inappropriately limit patient
access.
Make Mental Health and Substance Use Treatment A
Reality
The law currently requires health insurers to provide mental
health and substance use disorder benefits in parity with physical health benefits.
But in 2018, less than half of
people with mental illness received treatment and less than a fifth of people
who needed substance use treatment actually received it. As
president, I will launch a full-scale effort to enforce these requirements –
with coordinated actions by the IRS, Centers for Medicare and Medicaid
Services, and Department of Labor to make sure health plans actually provide
mental health treatment in the same way they provide other treatment.
Reverse Trump’s Sabotage
I will reverse the Trump administration’s actions that have
undermined health care in America. Key steps include:
Protecting coverage for people with pre-existing
conditions. The Trump administration has abandoned its duty
to defend current laws in court, cheering on efforts to destroy protections for
pre-existing conditions, insurance coverage for dependents until they’re 26,
and the other critical Affordable Care Act benefits. In a Warren
administration, the Department of Justice will defend this law. And we will
close the loopholes created by the Trump administration, using 1332 waivers,
that could allow states to steer healthy people toward parallel, unregulated
markets for junk health plans. This will shut down a stealth attack on people
with pre-existing conditions who would see their premiums substantially
increase as healthier people leave the marketplace.
Banning junk health plans. The Trump
administration has expanded the use of
junk health insurance plans as an alternative to comprehensive health plans
that meet the standards of the ACA. These plans cover few benefits,
discriminate against people with pre-existing conditions, and increase costs
for everyone else. And in some cases they direct as much as 50 percent of
patient premiums to administrative expenses or profit. I will ban junk plans.
Expanding ACA enrollment. I’ll re-fund the
Affordable Care Act programs that help people enroll in ACA coverage, programs
that have been gutted by the Trump administration.
Expanding premium tax credits. I will reverse
the Trump administration rule that artificially reduced premium tax credits for
many people, making coverage less affordable –
and instead will expand these credits.
Rolling back Trump’s sabotage of Medicaid. I’ll
reverse the Trump administration’s harmful Medicaid policies that take coverage
away from low-income individuals and families. I’ll prohibit restrictive and
ineffective policies like work requirements – which have already booted 18,000 people in
Arkansas out of the program – as well as enrollment caps, premiums, drug
testing, and limits on retroactive eligibility that can prevent bankruptcy.
Restoring non-discrimination protections in health
care. I will immediately reverse the Trump administration’s
terrible proposed rule permitting
health plans and health providers to discriminate against women, LGBTQ+ people,
individuals with limited English proficiency, and others.
Ending the Trump administration’s assault on reproductive
care. I’ll roll back the Trump administration’s domestic and global
gag rules, which deny Title X and USAID funding to health care providers who
provide abortion care or even explain where and how patients can access safe,
legal abortions. And I will overturn the Trump administration’s embattled proposed rule to
roll back mandatory contraceptive coverage.
Strengthen the Affordable Care Act
As president I will use administrative tools to strengthen
the ACA to reduce costs for families and expand eligibility. Key steps include:
Stop families from being kicked out of affordable
coverage. Because of something called the “family glitch,” an
entire family can lose access to tax credits that would help them buy health
coverage if one parent is offered individual coverage with a premium less than
9.86% of their family income. I’ll work to make sure that a family’s access to
tax credits is based on the affordability of coverage for the whole family –
not just one individual – so families who don’t actually have access to
affordable alternatives don’t lose their ACA tax credits.
Expand eligibility to all legally present
individuals. I’ll also work to extend eligibility for ACA tax credits
to all people who are legally present, including those eligible for the
Deferred Action for Childhood Arrivals program.
Put money back in workers’ pockets. The
Affordable Care Act requires insurance
companies to spend at least 80 percent of total premium contributions on health
care claims (and, in many cases, at least 85 percent), leaving the rest to be
spent on plan administration, marketing, and profit. Insurers who waste money
must issue rebates – but too often, these are returned to employers who don’t pass
on the savings to their employees. Insurance companies are expected to pay
out $1.3 billion in
rebates in 2019, with employers in the small-group market receiving an average
rebate of $1,190 and employers in the large-group market receiving an average
rebate of $10,660. My plan will require employers to pass along the full value
of the rebate directly to employees.
Strengthen Medicare
As president I will use administrative tools to strengthen
Medicare:
Expand Dental Benefits. The Medicare statute
prohibits coverage of dental care that is unrelated to other medical care,
unless it is medically necessary. This has been interpreted to largely exclude
any oral health care. As a result, almost two-thirds of
Medicare beneficiaries, or nearly 37 million people, lack access to dental
benefits. I will use my administrative authority to clearly expand the
medically necessary dental services Medicare can provide, improving the health
of millions of Medicare beneficiaries.
Stop private Medicare Advantage plans from bilking
taxpayers. Roughly one-third of Medicare beneficiaries get coverage
through a private Medicare Advantage plan. Medicare payments to these plans for
each enrollee are supposed to reflect the cost of covering that person through
traditional Medicare, but overwhelmingevidence shows that
these private plans make their enrollees appear sicker on paper than they
actually are to earn inflated payments at the expense of taxpayers. Some suggest that this
adds $100 billion or more to Medicare spending over ten years. My
administration will put an end to this fraud.
Strengthen Medicaid
As president I will use administrative tools to strengthen
Medicaid and potentially allow millions more to access the program.
Use waiver authority to increase Medicaid eligibility. With
the approval of the federal government, states can use Section 1115
demonstration waivers to expand coverage to people who aren’t otherwise
eligible for Medicaid. Currently, however, states can only obtain these waivers
if projected federal spending under the new program will not be higher than without the
waiver. While I pursue legislative reforms to expand coverage, I’ll
also change this administrative restriction to allow these demonstrations to
fulfill their promise of providing affordable health coverage, including
working with states that want to expand Medicaid to uninsured individuals and
families above the statutory upper limit of Medicaid (138% of the poverty
level). Any state that chooses to expand in this way will not be penalized for
doing so when full Medicare for All comes online.
Streamlining eligibility and enrollment. Far too
many people miss out on Medicaid coverage because of red tape. Some states take
coverage away if someone misses just one piece of mail or forgets to notify the
state within 10 days of a change in income. These kinds of harsh policies help
explain why more than a million children “disappeared” from the
Medicaid and CHIP programs in the past year. I will eliminate these kinds of
unfair practices, and instead work with states to make it easier for everyone –
families, children, and people with disabilities – to maintain this essential
coverage.
Ensuring access to care for beneficiaries in managed care
plans. I’ll roll back the Trump administration’s proposed changes to
rules regulating Medicaid managed care plans, which would dilute important
standards, such as requiring health plans to maintain adequate provider
networks guaranteeing access to care for Medicaid enrollees.
Antitrust Enforcement for Hospitals and Health
Systems
For years, both horizontal
mergers (where hospitals purchase other hospitals) and vertical mergers (where
hospitals acquire physician practices) have produced greater hospital and
health system consolidation, contributing to the skyrocketing costs of health
care. Today, “not a single
highly competitive hospital market remains in any region of the United
States.” Study after studyshowsthat mergers mean higher prices, lower quality,
and increased inequality due to the growing wage gap between
hospital CEOs and everyone else. Bringing down the cost of health care means
enforcing competition in these markets.
As president, I will appoint aggressive antitrust enforcers
who recognize the problems with hospital and health system consolidation to the
Department of Justice and Federal Trade Commission. My administration will also
conduct retrospective reviews of significant new mergers, and break up mergers
that should never have taken place.
Bringing Health Records into the 21st Century
Congress spent $36 billion to get
every doctor in America using electronic health records, but we still do not have adequate digital
information flow in health care – in part because two big
companies make up about 85% of the market for
medical records at big hospitals. As they attempt to capture more of the
market, these companies are making it harder for systems to communicate with each other. My
administration will ramp up the enforcement against information blocking by big
hospital systems and health IT companies, and I will appoint leaders to the FTC
and DOJ who will conduct a rigorous antitrust investigation of the health
records market, especially in the hospital space.
Elevating the Voices of Workers in the Transition to
Medicare for All
The fundamental goal of my presidency will be returning
power to working people. Medicare for All accomplishes that by giving every
American high-quality coverage and freeing them from relying on the whims of
their employers or private insurance companies for the health care they need.
My plan to transition to Medicare for All will also put working people first,
and elevate their voices at each stage of the process.
My plan seeks to build on the achievements of generations of
working people and their unions who have fought for and won health care. I view
good health plans negotiated through collective bargaining as a positive
achievement for working people, and I will seek as part of the first phase of
my plan the elimination of the excise tax on those plans.
In my first weeks in office, I will issue an Executive Order
creating a commission of workers (including health care workers), union
representatives, and union benefit managers that I will consult at every stage
of the transition process. The commission will be responsible for providing
advice on each element of the transition to Medicare for All, including, at a
minimum:
Ensuring workforce readiness and adequate access to care
across all provider types.
Determining national standards of coverage and benefits,
including long-term care.
Learning from successful existing non-profit health care
administrators and integrating them into the new Medicare for All system.
Ensuring a living wage for all health care workers and that
savings generated within the new system by hospitals and other health care
employers are shared fairly with all of the workers in the health care system.
Ensuring that workers are able to use the collective
bargaining process during the transition period and under the new Medicare for
All system to ensure both effective health outcomes and to ensure that savings
generated by the new system are fairly shared with workers.
In administering the Medicare for All system, my
administration will also rely on unions’ expertise on designing good benefits
for workers and helping workers navigate our health care system. During the
transition to Medicare for All – and even when we ultimately reach a full
Medicare for All system – my administration will seek to partner with
collectively bargained non-profit health care administrators. For example, we
will draw upon their expertise in helping workers choose providers, and look
for opportunities to enter into contracts with the administrators of unions’ collectively
bargained health plans to provide these services. And my plan will guarantee
that union-sponsored clinics are included within the Medicare for All system
and will continue serving their members.
Finally, Medicare for All will be an enormous boost to
the economy, lifting a weight off of both workers and businesses and creating
good new jobs, including in administering health care benefits. Still, the
Medicare for All legislation includes billions of dollars to provide assistance
to workers who may be affected by the transition to Medicare for All, and I
plan on consulting with the new worker commission and other affected parties to
ensure that money is spent as effectively as possible. In the past, transition
assistance programs have been underfunded and have not been as responsive as
they should have been to the actual needs of workers. That will not be the case
in my administration. No worker will be left behind.
Legislation to Expand Medicare and Create a True Medicare
for All Option
In 2017, Senate Republicans came within one vote of
shredding the Affordable Care Act and taking health care coverage away from
more than 20 million people. How did they get so close? By using a fast-track
legislative process called budget reconciliation, which only requires 50 votes
in the Senate to pass laws with major budgetary impacts. President Obama also
used this process to secure final passage of the Affordable Care Act.
I am a strong supporter of eliminating the filibuster, which
I believe is essential to preventing right-wing Senators who function as wholly
owned subsidiaries of major American industries from blocking real legislative
change in America. Any candidate for president who does not support this change
should acknowledge the extreme difficulty of enacting their preferred
legislative agenda. But I’m not going to wait for this to happen to start
improving health care – and I’m not going to give Mitch McConnell or the
Republicans a veto over my entire health care agenda.
That’s why, within my first 100 days, I will pass my own
fast-track budget reconciliation legislation to enact a substantial portion of
my Medicare for All agenda – including establishing a true Medicare for All
option that’s free for millions and affordable for everyone.
A True Medicare for All Option. There are many
proposals that call themselves a Medicare for All “public option” – but most of
them lack the financing to actually allow everyone in America to choose true
Medicare for All coverage. As a result, these proposals create the illusion of
choice, when in reality they offer tens of millions of Americans the decision
between unaffordable private insurance and unaffordable public insurance. A
choice between two bad options isn’t a choice at all.
My approach is different.
Because I have identified trillions in revenue to finance a
fully functioning Medicare for All system – without raising taxes on the middle
class by one penny – I can also fund a true Medicare for All option. The plan
will be administered by Medicare and offered on ACA exchanges. Here are its key
features:
Benefits. Unlike public option plans, the
benefits of the true Medicare for All option will match those in the Medicare
for All Act. This includes truly comprehensive coverage for primary and
preventive services, pediatric care, emergency services and transportation,
vision, dental, audio, long-term care, mental health and substance use, and
physical therapy.
Immediate Free Coverage for Millions. This plan
will immediately offer coverage at no cost to every kid under the age of 18 and
anybody making at or below 200% of the federal poverty level (about $51,000 for
a family of four) – including individuals who would currently be on Medicaid,
but live in states that refused to expand their programs.
Free, Identical Coverage for Medicaid
Beneficiaries. States will be encouraged to begin paying a
maintenance-of-effort to the Medicare for All option in exchange for moving
their Medicaid populations into this plan and getting out of the business of
administering health insurance. For states that elect to maintain their
Medicaid programs, Medicaid premiums and cost sharing will be eliminated, and
we will provide wraparound benefits for any Medicare for All option benefits
not covered by a state’s program to ensure that these individuals have the same
free coverage as Medicaid-eligible people in the Medicare for All option.
Eventual Free Coverage for Everyone. This plan
will begin as high-quality public insurance that covers 90% of costs and allows
people to utilize improved ACA subsidies to purchase coverage and reduce cost
sharing. There will be no premiums for kids under 18 and people at or below
200% of the federal poverty level. For individuals above 200% FPL, premiums
will gradually scale as a percentage of income and are capped at 5.0% of their
income. Starting in year one, the plan will not have a deductible — meaning
everyone gets first dollar coverage, and cost sharing will be zero for people
at or below 200% FPL. Cost sharing will scale modestly for individuals at or
above that level, with caps on out-of-pocket costs. In subsequent years,
premiums and cost sharing for all participants in this plan will gradually
decrease to zero.
Reducing Drug Prices. The Medicare for All
option will have the ability to negotiate for prescription drugs using the
mechanisms I’ve previously outlined,
helping to drive down costs for patients.
Automatic Enrollment. Anyone who is uninsured or
eligible for free insurance on day one, excluding individuals who are over 50
and eligible for expanded coverage under existing Medicare, will be
automatically enrolled in the Medicare for All option. Individuals who prefer
other coverage can decline enrollment.
Employee Choice. Workers with employer coverage
can opt into the Medicare for All option, at which point their employer will
pay an appropriate fee to the government to maintain their responsibility for
providing employee coverage. In addition, unions can negotiate to include a
move to the Medicare for All option via collective bargaining during the
transition period, with unionized employers paying a discounted contribution to
the extent that they pass the savings on to workers in the form of increased
wages, pensions, or other collectively-bargained benefits. This will support
unions and ensure that the savings from Medicare for All are passed on to
workers in full, not pocketed by the employer.
Provider Reimbursement and Cost Control. I
have identified cost
reforms that would save our health system trillions of dollars when implemented
in a full Medicare for All system. The more limited leverage of a Medicare for
All option plan will accordingly limit its ability to achieve these savings –
but as more individuals join, this leverage will increase and costs will go
down. Provider reimbursement for this plan will start above current Medicare
rates for all providers, and be reduced every year as providers’ administrative
and delivery costs decrease until they begin to approach the targets in my
Medicare for All plan. The size of these adjustments will be governed by
overall plan size and the progress of provider adjustment to new, lower
rates.
Expand and Improve Existing Medicare for Everyone Over
50. In addition to the Medicare for All option, any person over the
age of 50 will be eligible for expanded coverage under the existing Medicare
program, whose infrastructure will allow it to absorb new beneficiaries more
quickly. The expanded Medicare program will be improved in the following
ways:
Benefits. To the greatest extent possible,
critical benefits like audio, vision, full dental coverage, and long-term care
benefits will be added to Medicare, and we will legislate full parity for
mental health and substance use services.
Eventual Free Coverage for Everyone. Identical
to the Medicare program, enrollees will pay premiums in Part B and D, with a
$300 cap on drug costs in Part D. Plugging a huge hole in the current Medicare
program, out-of-pocket costs will be capped at $1,500 per year across Parts A,
B, and D, eliminating deductibles and reducing cost sharing. In subsequent
years, premiums and cost sharing will gradually decrease to zero.
Employee Choice. Identical to the Medicare for
All option, workers 50-64 can opt into expanded Medicare, at which point their
employer will pay an appropriate fee to the government to maintain their
responsibility for providing employee coverage.
Reducing Drug Prices. The expanded Medicare
program will receive the ability to negotiate for prescription drugs using the
mechanisms I’ve previously outlined,
helping to drive down costs for patients. And we will create a publicly run
prescription drug plan that is benchmarked off the best current Part D
plan.
Automatic Enrollment. Every person without
health insurance over the age of 50 will be automatically enrolled in the
expanded existing Medicare program.
Provider Reimbursement and Cost Control. Provider
reimbursement for new beneficiaries will start above current Medicare rates for
all providers, and be reduced every year as providers’ administrative and
delivery costs decrease until they begin to approach the targets in my Medicare
for All plan. It will be a new condition of participation that providers who
take Medicare or other federally subsidized insurance also take the Medicare
for All option. We will also adopt common sense reforms to bring down bloated
reimbursement rates, including reforms around post-acute care, bundled
payments, and site neutral payments.
Improving the Affordable Care Act. My reforms
will also strengthen Affordable Care Act plans – including the new Medicare for
All option – by making the following changes:
Expand Tax Credit Eligibility. We will lift the
upper limit on eligibility for Premium Tax Credits, allowing people over 400%
of the federal poverty level to purchase subsidized coverage and greatly
increasing the number of people who receive subsidies.
Employee Choice. We will allow any person or
family to receive ACA tax credits and opt into ACA coverage, regardless of
whether they have an offer of employer coverage. If an individual currently
enrolled in qualifying employer coverage moves into an ACA plan, their employer
will pay an appropriate fee to the government to maintain their responsibility
for providing employee coverage.
Lower Costs. Right now, people may pay up to 9.86% of their
income before they get subsidies. Under my plan, this cap would be lowered –
and to make sure those tax credits cover more, we will benchmark them to more
generous “gold” plans in the Marketplace. And we will increase eligibility for
cost sharing reductions, ensuring that more individuals can get into an
affordable exchange plan immediately.
Eliminate the Penalty for Getting a Raise. Right
now, if someone’s income goes up, they can be forced to repay thousands of
dollars in back premiums. We will change this and base tax credits on the
previous year’s income. And if someone’s income goes down, they will get the
higher subsidy for that year.
State Single-Payer Innovation Waivers. To help
states try out different payer arrangements and pilot programs, we will allow
states to receive passthrough funding to expand or improve coverage via the
ACA’s Section 1332 waivers. Combined with Medicaid waivers, these changes will
allow interested states to start experimenting immediately with consolidating
public payers and move towards a single-payer system.
Additional Financing. My plan to pay for
Medicare for All identifies $20.5 trillion in new revenue, including an
Employer Medicare Contribution, which will cover the long-term, steady-state
cost of a fully functioning Medicare for All system. The cost of this
intermediate proposal will be lower. Any revenue needed to meet the
requirements of fast-track budget reconciliation will be enacted as part of
this legislation from the financing options that I have already proposed.
Additional Health System Reforms to Save Money and Lives
After pursuing administrative changes, expanding existing
Medicare, and creating a true Medicare for All option, every person in the
United States will be able to choose free or low-cost public insurance. Tens of
millions will likely do so. But we can’t stop there. We must pursue additional
reforms to our health system to save money and save lives. Some of my
priorities include:
Investing in Medical Miracles. Many medical
breakthroughs stem from federal investments in
science – but in 2018, 43,763 out of 54,834 research
project grant applications to the National Institutes of Health (NIH) were
rejected. We will boost medical research by investing an additional $100
billion in guaranteed, mandatory spending in the NIH over ten years, split
between basic science and the creation of a new National Institute for Drug
Development that will help take the basic research from the other parts of NIH
and turn it into real drugs that patients can use. We will prioritize
treatments that are uninteresting to big pharmaceutical companies but could
save millions of American dollars and lives. Any drugs that come out of this
research and to American consumers can be sold abroad, with the proceeds
reinvested to fund future breakthrough drug development. And by enacting my
Affordable Drug Manufacturing Act, the government can manufacture generic drugs
that are not available due to cost or shortage.
Ending the Opioid Epidemic. The opioid epidemic
is a public health emergency. In 2017, life expectancy in the United States
dropped for the third year in a row, driven in large part by deaths from drug
overdoses. We will enact my legislation, the CARE Act, to invest $100 billion
in federal funding over the next ten years in states and communities to fight
this crisis – providing resources directly to first responders, public health
departments, and communities on the front lines of this crisis.
Improved Administration. To cut down on time
wasted on paperwork, we will create single standardized forms for things like
prior authorizations and appeals processes to be used by all insurers (private
and public), and we will establish uniform medical billing for insurers and
doctors.
All-Payer Claims Database. Right now, there are so
many middlemen in health care that no one knows for certain how much we pay for
different services across the whole system. A centralized repository of
de-identified claims data will help the government, researchers, and the market
better understand exactly what we pay for health care and what kind of quality
it gets us. Demystifying what we pay for what we get will be a critical part of
ensuring fair reimbursement under Medicare for All.
Antitrust Enforcement. In addition to
administrative actions to rein in anti-competitive hospital and electronic
medical record practices, we’ll also ban non-compete and no-poach agreements
and class action waivers across the board, while making it easier for private
parties to sue to prevent anti-competitive actions. I’ll work with states to
repeal Certificate of Public Advantage, or COPA, statutes
that shield health care
organizations from federal antitrust review and can lead to the
creation of large monopolies with little to no oversight. And I’ll also push to
ensure our antitrust laws apply to all health care mergers.
Ending Surprise Billing. Imagine being a woman
who schedules her baby’s delivery with her obstetrician at an in-network
hospital, but it turns out that the anesthesiologist administering the epidural
isn’t in-network. Even though she had no choice – and probably had no idea that
doctor was out-of-network – under the current system she gets hit with a huge
bill. We will end the practice of surprise billing by requiring that
services from out-of-network doctors within in-network hospitals, in addition
to ambulances or out-of-network hospitals during emergency care, be treated as
in-network and paid either prevailing in-network rates or 125% of the Medicare
reimbursement rate, whichever is lower.
Preventing Provider Shortages. With more people
seeking the care they need, it will be essential to increase the number of
providers. I will make these
critical investments in our clinicians, including by dramatically scaling up
apprenticeship programs to build a health care workforce rooted in the
community. I will lift the cap on residency placements, allowing 15,000 new
clinicians to enter the workforce. I will expand the National Health Service
Corps and Indian Health Service loan repayment program to allow more health
professionals – including physicians, physician assistants, registered nurses,
nurse practitioners, and other licensed practitioners – to practice in
underserved communities. I will also provide grants to states that expand
scope-of-practice to allow more non-physicians to practice primary care. And I
will push to close the
mental health provider gap in schools.
Completing the Transition to Medicare For All
By pursuing these changes, we will provide every person in
America with the option of choosing public coverage that matches the full
benefits of Medicare for All. Given the quality of the public alternatives,
millions are likely to move out of private insurance as quickly as
possible.
No later than my third year in office, at which point the
number of individuals voluntarily remaining in private insurance would likely
be quite low, I will fight to pass legislation to complete the transition to
the Medicare for All system defined by the Medicare for All Act by the end of
my first term in office.
Moving to this system would mean integrating everyone into a
unified system with zero premiums, copays, and deductibles. Senator Sanders’s
Medicare for All Act allows for supplemental private insurance to cover
services that are not duplicative of the coverage in Medicare for All; for
unions that seek specialized wraparound coverage and individuals with
specialized needs, a private market could still exist. In addition, we can
allow private employer coverage that reflects the outcome of a collective
bargaining agreement to be grandfathered into the new system to ensure that
these workers receive the full benefit of their bargain before moving to the
new system. But the point of Medicare for All is to cut out the middleman.
Every successful effort to move the United States to create
and expand new social programs – like Social Security and Medicare and Medicaid –
has required multiple steps. In fact, every credible Medicare for All proposal
has a significant, multi-step transition built in. That’s why it’s important to
have both short-term goals and long-term goals to guide the process and to
deliver concrete improvements to people’s lives at every stage.
I believe the next president must do everything she can
within one presidential term to complete the transition to Medicare for All. My
plan will reduce the financial and political power of the insurance companies –
as well as their ability to frighten the American people – by implementing
reforms immediately and demonstrating at each phase that true Medicare for All
coverage is better than their private options. I believe this approach gives us
our best chance to succeed.
Why do we need to transition to Medicare for All if a robust
Medicare for All option is available to everyone? The answer is simple and
blunt: cost and outcomes. Today, up to 30% of
current health spending is driven by the costs of filling out different
insurance forms and following different claims processes and fighting with
insurance companies over what is and is not covered. I have demonstrated how a
full Medicare for All system can use its leverage to wring trillions of dollars
in waste out of our system while delivering smarter care – and I’ve made clear exactly
how I would do it. The experience of other countries shows that this system is
the cheapest and most efficient way to deliver high-quality health care. As
long as duplicative private coverage exists, we will limit our ability to make
health care delivery more effective and affordable – and the ability of private
middlemen to abuse patients will remain.
Medicare for All will deliver an $11 trillion boost to
American families who will never pay another premium, co-pay, or deductible.
That’s like giving the average working family in America a $12,000 raise. This
final legislation will put a choice before Congress – maintain a two-tiered
system where private insurers can continue to profit from being the middlemen
between patients and doctors, getting rich by denying care – or give everybody
Medicare for All to capture the full value of trillions of dollars in savings
in health care spending. I believe that the American people will demand
Congress make the right choice.
Senator Elizabeth Warren, Democratic candidate for President, has released details of her most controversial proposal, Medicare for All, promising that it will cover every person in America with health care, including long-term care, vision and dental, without increasing taxes on middle class families. Warren focuses on an overall restructuring taxes and spending – going after the loopholes and tax cheats and reining in military spending as well as drug costs and cutting healthcare costs by removing the for-profit insurance companies (gatekeepers) as middlemen. What her plan misses, though, is the obvious: collect the Medicare tax (1.45%, plus an extra 0.9% on income over $200,000) on all income, not just wages, and, if necessary raise the surcharge for incomes over $250,000. Interestingly, while employers would no longer pick and choose the private health insurance they subsidize, employers would still subsidize their employees’ Medicare cost. Health care is considered the leading issue for voters in 2020. Here is the detailed plan, from the Warren campaign: –Karen Rubin/news-photos-features.com.
Charlestown, MA
– Today, Senator Elizabeth
Warren, candidate for President, released her plan to finance Medicare for All.
The coverage is identical to the coverage in the Medicare for All legislation
in the Senate and it will cover every single person in America with excellent,
high-quality health care, including long-term care and vision and dental.
Elizabeth will pay
for this plan without raising taxes one penny on middle class families. Instead, she will put about $11
trillion in the pockets of American families by eliminating what they would pay
in premiums, deductibles, co-pays, and other out-of-pocket costs over the next
ten years.
Her numbers add up and
are backed by experts including:
Simon Johnson, the
former Chief Economist at the International Monetary Fund and a professor at
MIT
Dr. Donald Berwick,
one of the nation’s top experts in health system management and improvement,
who ran the Medicare and Medicaid programs under President Barack Obama
Mark Zandi, Chief
Economist of Moody’s Analytics
Betsey Stevenson,
former Chief Economist for the Obama Labor Department
Elizabeth’s plan to
dramatically improve health care and cut family costs would cost the United
States less than our current broken system. It would require $20.5 trillion in
new revenue, nearly half of which comes simply from having employers pay
Medicare instead of private insurance companies.
Elizabeth will finance
the remainder of Medicare for All with targeted defense spending cuts, new
taxes on financial firms, giant corporations, and the richest 1% of Americans,
and by cracking down on tax evasion and fraud. The $11 trillion in household
insurance and out-of-pocket expenses projected under our current system goes
right back into the pockets of America’s working people — substantially larger than the
largest tax cut in American history — and no middle class tax increases.
My daddy’s heart attack nearly sent our family skidding over
a financial cliff. Today I think about all the kids this year who will face the
double blow of nearly losing a parent and then watching their lives turn upside
down as their families struggle to pay a growing stack of medical
bills.
I spent my career studying why so many hard-working middle
class families were going broke. For years, my research partners and I traveled
the country from bankruptcy courtroom to bankruptcy courtroom, talking directly
to people who’d seen their lives turned upside down. We interviewed lawyers,
judges, and families involved in bankruptcy cases. To save on printing costs,
we lugged around a Xerox machine (I nicknamed him “R2-D2”) to save money on
photocopying court records.
Eventually, we built the largest and most comprehensive
database of consumer bankruptcy data ever assembled. That first study surprised
us: we found that 90% of families went bankrupt because of job loss, medical
problems, and marital disruption. That finding was confirmed in 2007 by my
later research, which found that the number one reason
families were going broke was health care – and three quarters of
those who declared bankruptcy after an illness were people who already had
health insurance.
It’s been nearly thirty years since we published that first
groundbreaking study. And after all that time, here’s where we are: between
2013 and 2016, the number one reason families
went broke was still because of health care – even though 91.2% of Americans
had health insurance in 2016.
Families are getting crushed by health costs. Just look at
the numbers.
$12,378. That’s
how much an average family of four with employer-sponsored insurance personally
spent per year on employee premium contributions and out-of-pocket
costs in 2018. And this figure has increased each
year.
87 million. That’s
how many American adults in 2018 were uninsured or “underinsured” – meaning
either they have no insurance or their so-called health insurance is like a car
with the engine missing. It looks fine sitting on the lot, but inadequate if
they actually need to use it. Nearly one in every
two adults not currently on Medicare has no insurance or unreliable insurance.
37 millionAmerican
adults didn’t fill a prescription last year because of costs. 36 millionpeopleskipped
a recommended test, treatment, or follow-up because of costs. 40 millionpeople
didn’t go to a doctor to check out a health problem because of costs. 57 millionpeople
had trouble covering their medical bills.
Today, in 2019, in the United States of America, the
wealthiest nation in the history of the world, inadequate health coverage is
crushing the finances and ruining the lives of tens of millions of American
families.
I’m running for President based on a radical idea – calling
out what’s broken and speaking plainly about how to fix it.
All my plans start with our shared values. There are two
absolute non-negotiables when it comes to health care:
One: No American should ever, ever die or go bankrupt
because of health care costs. No more GoFundMe campaigns to pay for care. No
more rationing insulin. No more choosing between medicine and groceries.
Two: Every American should be able to see the doctors they
need and get their recommended treatments, without having to figure out who is
in-network. No for-profit insurance company should be able to stop anyone from
seeing the expert or getting the treatment they need.
Health care is a human right, and we need a system that
reflects our values. That system is Medicare for All.
Let’s be clear: America’s medical professionals are among
the best in the world. Health care in America is world-class. Medicare for All
isn’t about changing any of that.
It’s about fixing what is broken – how we pay for that care.
And when it comes to health care, what’s broken is obvious.
A fractured system that allows private interests to profiteer off the health
crises of the American people. A system that crushes our families with costs
they can’t possibly bear, forcing tens of millions to go without coverage or
to choose between basic
necessities like food, rent, and health – or bankruptcy.
We must fix this system. And over the long-term, the best
way to achieve that goal is to move from the system we have now to a system of
Medicare for All.
Medicare for All is about where doctors, hospitals, and care
providers send the bill – to a collection of private insurance companies who make billions off
denying people care or to the Medicare program for fair compensation. Under
Medicare for All, everyone gets the care they need, when they need it, and
nobody goes broke.
A key step in winning the public debate over Medicare for
All will be explaining what this plan costs – and how to pay for it. This task
is made a hundred times harder by powerful health insurance and drug companies
that makebillions of dollars
off the current bloated, inadequate system – and would be perfectly happy to
leave things exactly the way they are.
In 2017 alone, health industry players whose profiteering
would end under Medicare for All unleashed more than 2,500 lobbyists on
Washington. These industries will spendfreely on shady TV
ads and lobbying to convince people that a program that saves them massive
sums of money will somehow cost them money.
That being able to see the doctors and get the treatments they need regardless
of what their employer or
their insurance company thinks
is somehow actually a loss of choice. That a program that covers more services,
more people, and costs the American people less than what we
currently spend on health care is somehow too expensive.
Meanwhile, where are the 2,500 lobbyists for the people who
get sick and can’t pay their medical bills? Where are the hundreds of
millions being spent so that people who are trying to balance a budget around
rising health care premiums and growing deductibles and copays can make their
voices heard in Washington? Washington hears plenty from the giant health
insurance and giant drug industries, but not so much from families being
squeezed to the breaking point.
So let’s focus on families’ expenses and families’ health
care.
Start with the Medicare for All Act – which
I have cosponsored. The bill provides a detailed proposal for how to achieve
our end goal. But as economists and advocates have noted, the legislation
leaves open a number of key design decisions that will affect its overall cost,
and the bill does not directly incorporate specific revenue measures. While
much of this ambiguity results from the reasonable choice to delegate
significant implementation discretion to the Executive Branch, it has also
allowed opponents of
Medicare for All to make up their own price tags and try to scare middle class
families about the prospect of tax increases – despite the conclusions of expert after expert after expert that it is
possible to eventually move to a Medicare for All system that gives both high
quality coverage for everybody and dramatically lowers costs for middle class
families.
The best way to fight misinformation is with facts. That’s
why today, I’m filling in the details and releasing a plan that describes how I
would implement the long-term policy prescriptions of the Medicare for
All Act and how to pay for it.
Under my plan, Medicare for All will cover the full list of
benefits outlined in the Medicare for All Act, including long-term
care, audio, vision, and dental benefits. My plan will cover every single
person in the U.S., and includes common-sense payment reforms that make
Medicare for All possible without spending any more money overall than we spend
now.
My plan reflects careful, detailed analyses from key
national experts in health policy, tax policy, and economics. By filling in the
details, we can strip away all the misleading political attacks and make plain
the choice facing the American people:
Option 1: Maintain our current system, which will cost
the country $52 trillion over ten years. And under that current system
–
24 million people
won’t have coverage, and millions can’t get
long-term care.
63 million have
coverage gaps or substandard coverage that could break down if they actually
get sick. And millions who have
health insurance will end up going broke at least in part from medical costs
anyway.
Together, the American people will pay $11 trillion of
that bill themselves in the form of premiums, deductibles, copays,
out-of-network, and other expensive medical equipment and care they pay for
out-of-pocket – all while America’s wealthiest individuals and
biggest companies pay far
less in taxes than in other major countries.
Option 2: Switch to my approach to Medicare for All,
which would cost the country just under $52 trillion over ten
years. Under this new system –
Every person in America – all 331 million people
– will have full health coverage, and coverage for long-term care.
Everybody gets the doctors and the treatments they need,
when they need them. No more restrictive provider networks, no more insurance
companies denying coverage for prescribed treatments, and no more going broke
over medical bills.
The $11 trillion in
household insurance and out-of-pocket expenses projected under our current
system goes right back into the pockets of America’s working people. And we
make up the difference with targeted spending cuts, new taxes on giant corporations
and the richest 1% of Americans, and by cracking down on tax evasion and
fraud. Not one penny in middle-class tax increases.
That’s it. That’s the choice. A broken system that leaves
millions behind while costs keep going up and insurance companies keep sucking
billions of dollars in profits out of the system – or, for about the same
amount of money, a new system that drives down overall health costs and, on
average, relieves the typical middle class families of $12,400 in insurance
premiums and other related health care costs.
No middle class tax increases. $11 trillion in household
expenses back in the pockets of American families. That’s substantially larger than the
largest tax cut in American history.
Not every candidate for president supports moving to a
system of Medicare for All. Some who support Medicare for All will have
different ideas about how to finance and structure it. And everybody knows that
there must be a real transition. But you don’t get what you don’t fight for –
and my view is clear.
Every candidate who opposes my long-term goal of Medicare
for All should explain why the “choice” of private insurance plans is
more important than being able to choose the doctor that’s best for you without
worrying about whether they are in-network or not. Why it’s more important than
being able to choose the right prescription drug for you without worrying about
massive differences in copays. Why it’s more important than being able to
choose to start a small business or choose the job you want without worrying
about where your health care coverage will be coming from and how much it will
cost.
Every candidate who opposes my long-term goal of Medicare
for All should put forward their own plan to cover everyone, without costing
the country anything more in health care spending, and while putting $11
trillion back in the pockets of the American people by eliminating premiums and
virtually eliminating out-of-pocket costs. Or, if they are unwilling to do
that, they should concede that they think it’s more important to protect the
eye-popping profits of private insurers and drug companies and the immense
fortunes of the top 1% and giant corporations, rather than provide
transformative financial relief for hundreds of millions of American
families.
And every candidate who opposes my long-term goal of
Medicare for All should put forward their own plan to make sure every single
person in America can get high-quality health care and won’t go broke – and
fully explain how they intend to pay for it. Or, if they are unwilling to do
that, concede that their half-measures will leave millions behind.
And make no mistake – any candidate who opposes my long-term
goal of Medicare for All and refuses to answer these questions directly should
concede that they have no real strategy for helping the American people address
the crushing costs of health care in this country. We need plans, not
slogans.
THE COST OF MEDICARE FOR ALL
A serious conversation about how to pay for Medicare for All
requires, first, determining how much such a system would cost.
In recent years, several economists and think tanks have
attempted to estimate the cost of a single-payer system in the United States.
Those estimates consider how much our nation’s health care spending will change
over a ten year window, and range from a $12.5 trillion decrease
to a $7 trillion increase.
They also consider how much additional money the federal government would need
to fund this system, and those estimates range from a low of $13.5 trillion to a
high of $34 trillion over
ten years.
Because nobody can actually see the future, some of this
variation results from different assumptions about how parts of our health care
system might work differently under Medicare for All. But most of the
difference comes from policy choices. And while the Medicare for All
Act is clear about some of these choices – for example, generous
benefits, long-term care coverage, and virtually no out-of-pocket expenses – it
is silent on a number of really important ones. How much will we pay for
medical care and for prescription drugs? What do we do with the existing money
that states spend on Medicaid? How aggressively will we cut administrative
costs? Aggressive choices mean a lower total cost. Less aggressive choices
result in a higher total cost.
Serious candidates for president should speak plainly about
these issues and set out their plans for cost control – especially those who
are skeptical of Medicare for All. Because whether or not we make modest or
transformative changes to our health care system, cancer, diabetes, strokes,
Alzheimer’s, and Parkinson’s aren’t going to simply disappear. And without
leadership from the top, neither will the mushrooming cost of care in America
that’s bankrupting our families.
I’ve asked top experts to consider the long-term cost of my
plan to implement Medicare for All over ten years – Dr. Donald Berwick, one of
the nation’s top experts in health system improvement and who ran the Medicare
and Medicaid programs under President Obama; and Simon Johnson, the former
Chief Economist at the International Monetary Fund and a professor at MIT.
Their analysis begins with the assumptions of a recent study by the Urban
Institute and then examines how that cost estimate would change as certain new
key policy choices are applied. These experts conclude that my plan would slightly
reduce the projected amount of money that the United States would otherwise
spend on health care over the next 10 years, while covering everyone and giving
them vastly better coverage.
REDUCING INSURER ADMINISTRATIVE COSTS
The business model of private insurers is straightforward:
pay out less for medical care than they take in as premiums. This model is
located right in the center of our health care system, wasting huge amounts of
time and money documenting and arguing over who is owed what. Incredibly,
insurance companies spend a whopping $350 billion on
administration costs annually—and then, in turn, push huge additional
administrative costs onto hospitals, doctors, and millions of other health care
professionals in the from of complex billing—and then, in turn, drive up costs
incurred by employers as they attempt to navigate the complexity of providing
their employees with insurance.
Medicare for All will save money by bringing down the
staggering administrative costs for insurers in our current system. As the
experts I asked to evaluate my plan noted, private insurers had administrative
costs of 12% of premiums collected in 2017, while Medicare kept its
administrative costs down to 2.3%. My plan will ensure that Medicare for All
functions just as efficiently as traditional Medicare by setting net
administrative spending at 2.3%.
COMPREHENSIVE PAYMENT REFORM
In 2016, the United States spent nearly twice as
much on health care as ten high-income countries, and these costs have
been steadily rising for
decades, growing from 5.2%
of U.S. GDP in 1963 to 17.9% in 2017. But
instead of resulting in better health outcomes, Americans have the lowest
life expectancy of residents in high-income countries, the highest infant
mortality rate, and the highest obesity rates.
Why? As a group of health economists famously wrote, “It’s the prices,
stupid.”
Studieshave continued to
show that it’s not how much people use the health care system, often referred
to as “utilization,” but rather how much people pay that drives our high spending.
Compared to other high income countries, Americans simply pay more for health
care. We pay more for physicians and nurses. We pay more in administrative
costs. We pay more for prescription drugs.
A heart bypass surgery that costs nearly
$16,000 in the Netherlands costs an average of $75,000 in the United States. A
CT scan that costs $97 in Canada
costs an average of $896 here. And in the United States, hospitals can charge new parents
for holding their newborn after delivery.
Meanwhile, private equity firms fight bipartisan
legislation in Washington that might undermine the profitability of their
investments or prevent their hospitals from sending patients surprise bills.
And health care CEO salaries continue to soar. Between 2005 and 2015,
non-profit hospital CEO salaries increased by 93% to
an average of over $3 million, and last year, 62 health care CEOs raked in a
combined $1.1 billion – more
than the CDC spent on chronic disease prevention.
If we expect the American people to be able to afford health
care, we need to rein in these costs. Comprehensive payment reform, as part of
Medicare for All, will reduce this component of health care spending. Under my
approach, Medicare for All will sharply reduce administrative spending
and reimburse physicians and other non-hospital providers at current Medicare
rates. My plan will also rebalance rates in a budget neutral way that
increases reimbursements for primary care providers and lowers reimbursements
for overpaid specialties.
While private insurance companies pay higher rates, this system would be
expected to continue compensating providers at roughly the same overall rate
that they are currently receiving. Why? This is partially because providers
will now get paid Medicare rates for their Medicaid patients – a substantial
raise. But it’s also because providers spend an enormous amount of time on
billing and interacting with insurance companies that reduces their efficiency
and takes away from time with patients. Some estimate that hospitals will spend $210 billion on
average annually on these costs.
The nonpartisan Institute of Medicine estimates that
these wasted expenses account
for 13% of the revenue for physician practices, 8.5% for hospitals, and 10% for
other providers. Together, the improved efficiency will save doctors time and
money – helping significantly offset the revenue they will lose from
getting rid of higher private insurance rates.
Under my approach, Medicare for All will sharply
reduce administrative spending and reimburse hospitals at an average of 110% of
current Medicare rates, with appropriate adjustments for rural hospitals,
teaching hospitals, and other care providers with challenging cost structures.
In 2017, hospitals that treated Medicare patients were paid about 9.9% less than
what it cost to care for that patient. The increase I am proposing under
Medicare for All will cover hospitals’ current costs of care – but hospital
costs will also substantially decrease as a result of simpler administrative
processes, lower prescription drug prices, the end of bad debt from
uncompensated care, and more patients with insurance seeking care.
Of course, as Medicare currently recognizes,
not every provider situation is the same, and my Medicare for All program
maintains these base rate adjustments for geography and other factors. In
my plan for Rural
America, for example, I have committed to creating a new designation under
Medicare for rural hospitals due to the unique challenges health systems face
in rural communities. That’s why my plan allows for adjustments above the 110%
average rate for certain hospitals, like rural and teaching hospitals, and
below this amount for hospitals that are already doing fine with current
Medicare rates.Universal coverage will also have a
disproportionately positive effect on rural hospitals. Because people living in
rural counties are more likely to be
uninsured than people living in urban counties, these hospitals currently
provide a lot of uncompensated care. Medicare for All fixes that problem. And
I’ve previously laid out additional
investments to increase the number of Community Health Centers and grow our
health care workforce in rural and Native American communities, while cracking
down on anti-competitive mergers that lead to worse outcomes and higher costs
for rural communities.
We can also apply a number of common-sense, bipartisan
reforms that have been proposed for Medicare. Today, for example, insurers can
charge dramatically different prices for the exact same service based on where the service was
performed. Under Medicare for All, providers will receive the same
amount for the same procedure, saving hundreds of billions of dollars. We can
also make adjustments to things that we know Medicare currently pays too much
for – like post-acute care – by adjusting those payments down slightly while
accounting for the patient’s health status, bringing health care costs down
even more.
We will also shift payment rates so that we are paying for
better outcomes, instead of simply reimbursing for more services. We build on
the success of value-based reforms enabled by the Affordable Care Act,
including by instituting bundled payments for inpatient care and for 90 days of
post-acute care. Instead of paying providers for each individual service,
bundled payments reimburse providers for an entire “episode” of care and have
been shown to both improve outcomes and control costs. These
bundles help ensure that a patient’s different providers all communicate because
they are all tied to the same payment.
RESTORING HEALTH CARE COMPETITION
Health care consolidation has also contributed to
rising health care costs. One analysis found that over 90% of
metropolitan areas had health care provider markets that were either highly
concentrated or super concentrated in 2016. And despite the same kinds of empty
promises we see every time there’s industry consolidation – in this case, that
bigger hospitals would lead to better care – the data have not borne
this out. In fact, it’s theopposite: more
competition between providers creates incentives to improve care, and that
incentive will only increase under a
Medicare for All system where quality, not price, is the main differentiator in
the system.
Under Medicare for All, hospitals won’t be able to force
some patients to pay more because the hospital can’t agree with their insurance
company. Instead, because everyone has good insurance, providers will have to
compete on better care and reduced wait times in order to attract more
patients.
That’s why I will appoint aggressive antitrust enforcers to
the Department of Justice and Federal Trade Commission and allow hospitals to
voluntarily divest holdings to restore competition to hospital markets. I’ve
also previously committed to
strengthening FTC oversight over health care organizations, including
non-profit hospitals, to crack down on anti-competitive behavior. And I will
direct my FTC to block all future hospital mergers unless the merging companies
can prove that the newly-merged entity will maintain or improve care.
REINING IN OUT-OF-CONTROL PRESCRIPTION DRUG COSTS
Americans pay more for prescription drugs than anyone in the
world – $333 billion in
2017 alone. Americans spent $1,220 per person on
average for prescription drugs, while the next highest spending country,
Switzerland, spent $963 per person. That’s not because Americans use more
prescription medication – it’s because lax laws have allowed pharmaceutical
companies to charge insurance companies and patients exorbitant rates. In a
now-infamous example, when Turing Pharmaceuticals purchased the rights to the
HIV medication Daraprim, the company raised the price of
this life-saving drug from $13.50 per pill to a stunning $750 per tablet overnight.
The price of insulin has skyrocketed, forcing
people to risk their lives by rationing. And as prices continue to rise, more
Americans are turning to Canada in
search of affordable prices.
Reining in prescription drug costs should be a top priority
for any President – and there’s no better way to do it than through Medicare
for All. My administration will use a suite of aggressive policy tools to set a
net savings target that will bring down Medicare prices for brand name
prescription drugs by 70% and prices for generics by 30%, with an initial focus
on more expensive drugs.
Under Medicare for All, the federal government would have
real bargaining power to negotiate lower prices for patients. I will adopt an
altered version of the mechanism outlined in the Lower Prescription
Drug Costs Now Act which leverages excise taxes to bring manufacturers
to the table to negotiate prices for both branded and generic drugs, with no
drug exceeding 110% of the average international market price, but removes the
limit of the number of drugs Medicare can negotiate for and eliminates the
“target price” so Medicare could potentially negotiate prices lower than other
countries.
If negotiations fail, I will use two tools – compulsory
licensing and public manufacturing – to allow my administration to ensure
patient access to medicines by either overriding the patent, as modeled in
the Medicare Negotiation and Competitive Licensing Act, or by
providing public funds to support manufacturing of these drugs, as modeled in
my Affordable Drug Manufacturing Act. Medicare for All will also
incentivize pharmaceutical companies to develop the drugs we need – like
antibiotics, cancer cures, and vaccines. And it’s not just about driving down
drug prices. Making sure patients get important drug therapies up front that
keep them healthy and cost a fraction compared to more severe treatment down
the line can save money overall. Insurers, who may only cover individuals for a
few years of their lives, see those investments in long-term health as a cost
they’ll never recoup – so they have a financial incentive to deny patients these
treatments. But Medicare for All covers each patient for their entire lifespan.
There’s no perverse incentive to deny the prescriptions they need today because
the long-term benefits to their health won’t benefit their current private
insurance company.
STEMMING THE GROWTH OF MEDICAL COSTS
Year after year, U.S. health spending has grown at rates
above GDP growth, reaching a whopping 17.9% of GDP in
2017. Experts believe the changes to prescription drug spending and value-based
payment systems that I’ve already outlined will bring growth rates in line with
U.S. GDP, which CBO projects to be an average of 3.9% for
the next decade. And if growth rates exceed this rate, I will use available
policy tools, which include global budgets, population-based budgets, and
automatic rate reductions, to bring it back into line.
REDIRECTING TAXPAYER-FUNDED HEALTH SPENDING
Through Medicaid and public health plans for state
employees, state and local governments play a significant role in financing
health care coverage in America. Under my approach to Medicare for All, we will
redirect $6 trillion in existing state and local government insurance spending
into the Medicare for All system. This is similar to the mechanism that the
George W. Bush Administration used to redirect Medicaid spending to the federal
government under the Medicare prescription drug program.Under this
maintenance-of-effort requirement, state and local governments will redirect
$3.3 trillion of what they currently spend to support Medicaid and the
Children’s Health Insurance Program and $2.7 trillion of what they currently
spend on employer contributions to private insurance premiums for their
employees into Medicare for All. Because we bring down the growth rate of
overall health spending, states will pay less than they would have without
Medicare for All. They’ll also have far more predictable budgets, resulting in
improved long-term planning for state and community priorities.
Together, these policy choices represent significant
reductions in health care spending over current levels. Compared to the
estimate by the Urban Institute, they will save over $7 trillion over ten
years, bringing the expected share of additional federal revenue to just over
$26 trillion for that period. After incorporating the $6 trillion we will
redirect from states to help fund Medicare, the experts conclude that total
new federal spending required to enact Medicare for All will be $20.5 trillion.
PAYING FOR MEDICARE FOR ALL
Medicare for All puts all health care spending on the
government’s books. But Medicare for All is about the same price as our current
path – and cheaper over time. That means the debate isn’t really about
whether the United States should pay more or less. It’s about who should
pay.
Right now, America’s total bill for health care is projected
to be $52 trillion for the next ten years. That money will come from four
places: the federal government, state governments, employers, and individuals
who need care. Under my approach to Medicare for All, most of these funding
sources will remain the same, too.
Existing federal spending on Medicare and Medicaid will help
fund Medicare for All.
Existing state spending on health insurance will continue in
the form of payments to Medicare – but states would be better off because
they’d have more long-term predictability, and they’d pay less over time
because these costs will grow more slowly than they do today.
Existing total private sector employer contributions to
health insurance will continue in the form of contributions to Medicare – but
employers would be better off because under the design of my plan, they’d pay
less than they would have otherwise.
Here’s the main difference: Individual health care
spending.
Over the next ten years, individuals will spend $11 trillion
on health care in the form of premiums, deductibles, copays, and out-of-pocket
costs. Under my Medicare for All plan, that amount will drop from $11
trillion to practically zero.
I asked top experts – Mark Zandi, the Chief Economist of
Moody’s Analytics; Betsey Stevenson, the former Chief Economist for the Obama
Labor Department; and Simon Johnson – to examine options for how we can make up
that $11 trillion difference. They conclude that it
can be done largely with new taxes on financial firms, giant corporations, and
the top 1% – and making sure the rich stop evading the taxes we already have.
That’s right: We don’t need to raise taxes on the
middle class by one penny to finance Medicare for All.
Here’s how it would work.
REPLACING EMPLOYER HEALTH SPENDING WITH A NEW EMPLOYER
MEDICARE CONTRIBUTION
Let’s start with a basic fact: American companies are
already paying a lot for health care for their employees. They are projected to
pay nearly $9 trillion over the next ten years, mostly on employer
contributions for employee health insurance and on health-related expenses for
employees under workers’ compensation and long-term disability. My idea is that
instead of these companies sending those payments to private insurance
companies, they would send payments to the federal government for Medicare in
the form of an Employer Medicare Contribution.
In fact, it’ll be a better deal than what they have
now: companies will pay less than they otherwise would have, saving
$200 billion over the next ten years.
To calculate their new Employer Medicare Contribution,
employers would determine what they spent on health care over the last few
years and divide that by the number of employees of the company in those years
to arrive at an average health care cost per employee at the company.
(Companies would count part-time employees towards the total based on the
number of hours they worked during a year.) Under the first year of Medicare
for All, employers would then take that average cost, adjust it upwards to
account for the overall increase in national health care spending, and multiply
it by their total number of employees that year. Their Employer Medicare
Contribution would be 98% of that amount – ensuring that every company
paying for health care today will pay less than they would have if they were
still offering their employees comparable private insurance.
A similar calculation would apply to pass-through entities,
like law firms or private equity funds, even though many of the people that
work there technically aren’t employees. People who are self-employed would be
exempt from making Employer Medicare Contributions unless they exceed an income
threshold.
Small businesses – companies with under 50 employees – would
be exempt from this requirement too if they aren’t paying for employee health
care today. When either new or existing firms exceed this employee threshold,
we would phase in a requirement that companies make Employer Medicare Contributions
equal to the national average cost of health care per employee for every
employee at that company. Merging firms would pay the weighted average cost of
health care per employee of the two firms that are merging.
Employers currently offering health benefits under a
collective bargaining agreement will be able to reduce their Employer Medicare
Contribution if they pass along those savings to workers in the form of
increased wages, pensions, or other collectively-bargained benefits. New
companies or existing companies who enter into a collective bargaining
agreement with their employees after the enactment of Medicare for All will be
able to reduce their Employer Medicare Contributions in the same way. Employers
can reduce their contribution requirements all the way down to the national
average health care cost per employee.
That way, my plan helps unions that have bargained
for good health care already, and creates a significant new incentive for
unionization generally by making collective bargaining appealing for both
workers and employers as a way of potentially reducing the employer’s Employer
Medicare Contributions.
Over time, an employer’s health care cost-per-employee would
be gradually shifted to converge at the average health care cost-per-employee
nationally. That helps make sure the system is fair but also gives
employers and employees time to adapt to the new system.
If we’re falling short of the $8.8 trillion revenue target
for the next ten years, we will make up lost revenue with a Supplemental
Employer Medicare Contribution requirement for big companies with extremely
high executive compensation and stock buyback rates.
There are a variety of ways to structure an employer
contribution to Medicare for All. This particular approach has the benefit of
helping American employers in a few ways:
Employers would collectively save $200 billion over the next
ten years.
Employers receive far more certainty about how their health
care costs will vary over time and affect their finances.
Small businesses – who often suffer when competing for
employees because they can’t afford to
offer health care coverage – would no longer be at a competitive disadvantage
against bigger businesses.
Employers can reduce their Employer Medicare Contribution by
supporting unionization efforts and negotiating with workers to provide better
wages and benefits – reducing costs and promoting collective bargaining at the
same time.
Because my plan holds health care cost growth to GDP levels,
businesses will have stable balance sheets that grow with the economy instead
of crowding out other priorities.
By asking employers to pay a little less than what they
are already projected to pay for health care, we can get almost halfway to
where we need to go to cover the cost of my Medicare for All plan.
Automatic Increases in Take-Home Pay
Medicare for All puts a whole lot of money back in the
American people’s pockets. One way it does that is by taking the share of
premiums employees are responsible for paying through employer-sponsored
insurance – that line on pay stubs each week or month that says “health
insurance” – and returning it to working people. Congratulations on the
raise!
And higher take-home pay for workers also means additional
tax revenue just from applying our existing taxes – approximately $1.15
trillion if we apply average effective tax rates.
Medicare for All saves people money in other ways too. With
Medicare for All, nobody would need to put money in Health Savings Accounts or
medical savings accounts to try and protect themselves against the unthinkable.
And because individual spending on premiums, deductibles, copays, and
out-of-pocket costs will basically disappear, the tax break for medical
expenses in excess of 10% of Adjusted Gross Income becomes irrelevant.
Together, those changes would generate another
$250 billion in revenue.
All told, another $1.4 trillion in funding for Medicare for
All is generated automatically through existing taxes on the enormous amount of
money that will now be returned to individuals’ pockets from moving to a
Medicare for All system with virtually no individual spending on health
care.
Here’s what that means: we can generate almost half
of what we need to cover Medicare for All just by asking employers to pay
slightly less than what they are projected to pay today, and through existing
taxes.
So where does the rest of the money come from that allows us
to eliminate premiums, deductibles, copays, and most out-of-pocket spending for
every American? Four sources: (1) better enforcement of our existing tax laws
so we stop letting people evade their tax obligations; (2) targeted taxes on
the financial sector, large corporations, and the top 1% of individuals; (3) my
approach to immigration; and (4) shutting down a slush fund for defense
spending.
CRACKING DOWN ON TAX EVASION AND FRAUD
The federal government has a nearly 15% “tax gap”
between what it collects in taxes what is actually owed because of systematic
under-enforcement of our tax laws, tax evasion, and fraud. If that 15% gap
persists for the next ten years, we will collect a whopping $7.7 trillion less in
federal taxes than the law requires. By investing in stronger
enforcement and adopting best practices on tax reporting, withholding, and
filing, experts predict that we can close the tax gap by a third – generating
about $2.3 trillion in additional federal revenue without a single new
tax.
A big part of our current tax gap problem is that we’re letting
wealthier taxpayers get away with paying less than what they owe. Studies show that the
wealthiest 5% of taxpayers misrepresent their income more frequently than the
bottom 90%.
The wealthy and their allies in Washington have worked
to slash the IRS
budget, leaving it without the resources it needs. The agency today has about the
same number of revenue agents as it did when the economy was one-seventh its
current size in the 1950s. And the IRS insists on targeting low-income
taxpayers rather than wealthy ones, even though the amount of revenue we can
recover from wealthy taxpayers is far more.
We know how to fix this problem. We can draw lessons from
what works in other countries with much lower tax gaps and rely on the
recommendations of tax experts. Here’s a game plan:
Substantially increase funding for the IRS, including the
Criminal Investigation Division. The Treasury Department estimated in its
Fiscal Year 2017 budget request that every $1 invested in IRS enforcement
brings in nearly $6 in additional revenue – not even including an indirect
deterrence effect three times that amount.
Expand third-party reporting and withholding requirements.
Research shows that third-party reporting and withholding cuts down on the
tax misreporting rate substantially.
Strengthen enforcement of the Foreign Account Tax Compliance
Act (FATCA). FATCA requires foreign financial institutions to report the
holdings and income of U.S. taxpayers, but the IRS is generally not systematically matching these
reports to individual tax returns. We also don’t hold foreign financial firms
truly accountable for ignoring their reporting obligations. Automatically
matching FATCA reports to tax returns and instituting sanctions for
non-compliant foreign financial institutions would help narrow the tax gap.
Simplify tax filing obligations in line with other
comparable countries with lower tax gaps, including by adopting my Tax Filing Simplification Act and
using “smart returns” to
improve honest reporting.
Redirect enforcement resources away from low-income taxpayers towards
high-income taxpayers.
Increase the nonfiler compliance program, strengthen
reporting requirements for international income, use existing currency
transaction reports to enforce cash income compliance, and increase reporting
requirements for virtual- or crypto-currencies, as suggested by the
Treasury Department’s Inspector General.
Allow employees who
disclose tax evasion and abuse to use the protections of the False Claims Act
and other whistleblower protections.
The experts who reviewed these ideas estimated that if we
implemented them, we could close the tax gap by one-third from 15% to 10%,
bringing us closer to the tax gap in countries like the United Kingdom (5.6%). That will
produce another $2.3 trillion in net federal revenue – without imposing a
single new tax.
TARGETED TAXES ON THE FINANCIAL SECTOR, LARGE
CORPORATIONS, AND THE TOP 1%
We can generate a whole lot of the remaining revenue we need
for Medicare for All just by eliminating bad incentives in our current tax
system and asking those who have done really well in the last few decades to
pay their fair share.
Let’s start with the financial sector. It’s been more than
ten years since the 2008 financial crisis, and while a lot of families
are still dealing with
the aftereffects, the financial sector is making record, eye-popping profits.
Meanwhile, the risk of another financial crisis remains unacceptably high. By
imposing targeted taxes and fees on financial firms, we can generate needed
revenue and also make our financial system safer and more secure.
For example, a small tax on financial transactions –
one-tenth of one percent on the sale of bonds, stocks, or derivatives – would
generate about $800 billion in
revenue over the next ten years. The tax would be assessed on and
collected from financial firms, and would likely have little to no effect on
most investors. Instead, according to experts, the tax could
help decrease what Americans pay in fees for their investments and reduce the
size of relatively unproductive parts of the financial sector.
We can also impose a fee on big banks that encourages them
to take on fewer liabilities and reduce the risk they pose to the financial
system. A small fee that applies only to the forty or so largest banks in the
country would generate an additional $100 billion over
the next ten years – while making our financial system more safe and
resilient.
Next, we can make some basic changes to ensure that large
corporations pay their fair share and to fix some fundamental problems with our
current approach that actually encourage companies to shift jobs and investment
overseas. These changes will generate an estimated $2.9 trillion over
the next ten years.
For instance, our current tax system lets companies deduct
the cost of certain investments they make in assets faster than those assets
actually lose value. That means that if a company buys a machine for a million
dollars, it gets to deduct a million dollars from its taxes that same year –
even if the machine only loses $100,000 in value a year. Letting the company
write off the extra $900,000 all at once is like giving them an interest-free loan from
the government.
That might be worth it if the company responded to this tax
break by investing more and building out their businesses. But the datasuggest this isn’t
happening because companies don’t actually value these tax deferrals as much as
policymakers assume. Companies are mostly making the same investments they
would’ve made anyways – sometimes with small changes in timing – and getting a
write-off in exchange. Some experts even suggest that
accelerated expensing could induce less domestic investment,
not more.
That’s why I’m proposing to get rid of this loophole. Under
my plan, businesses will still write off the depreciation of their assets –
they’ll just do it in a way that more accurately reflects the actual loss in
value. This would generate $1.25 trillion over
ten years.
We can also stop giant multinational corporations from
calling themselves American companies while sheltering their profits in foreign
tax havens to avoid paying their share for American investments.
Currently, a U.S. multinational corporation can make
billions in profits and attribute it to a company it set up in a tax haven like
the Cayman Islands, which has no corporate taxes. The Trump tax bill claimed to
address that problem by creating a global minimum tax rate for corporations,
but that minimum tax – the result of heavy lobbying by
multinationals – is too low and easily gamed. While Trump and congressional
Republicans claimed their
minimum tax would keep companies from shifting profits to tax havens and limit
offshoring, the opposite is happening. The current
approach bothencourages companies
to shift their profits to tax havens and actually incentivizes American
companies to outsource their operations overseas.
That’s why I’m proposing to institute a country-by-country minimum
tax on foreign earnings of 35% – equal to a restored top corporate tax rate for
U.S. firms – without permitting corporations to defer those payments. Under
my plan, corporations would have to pay the difference between the minimum tax
and the rate in the countries where they book their profits. For example, an
American corporation booking a billion dollars in profits in the Cayman
Islands, taxed at 0% there, would need to pay the federal government a 35% tax
rate – the difference between the new minimum rate (35%) and the foreign rate
(0%) – on the billion dollars in profits.
My plan would also collect America’s fair share of profits
that foreign companies make by selling their products to Americans. Today, we
have a “global tax deficit”: companies that sell their goods abroad don’t have
to pay the extra taxes that they would have to pay if they were subject to a
minimum effective tax rate in each country they operated in. Making U.S. firms
pay a country-by-country minimum tax effectively collects their whole global
tax deficit – but foreign companies should have to pay their fair share, too.
That’s why I’m proposing that the U.S. collect the fraction of this global tax
deficit that corresponds to the percentage of that company’s sales in the U.S.
In other words, if a foreign company should owe an additional $1 billion in
taxes if it were subject to a country-by-country minimum tax, the U.S. would
collect a fraction of that $1 billion based on the amount of sales that company
made in the United States.
Together, the country-by-country minimum tax and the
taxation of foreign firms based on their domestic sales would result in an
additional $1.65 trillion in
revenue.
Finally, we can raise another $3 trillion over ten years by
asking the top 1% of households in America to pay a little more.
The tax burden on ultra-millionaires and billionaires is
less than half that of working families in the United States. In 2019, the
bottom 99% of families will pay 7.2% of their wealth
in taxes, while the top 0.1% of households will pay just 3.2%. My Ultra-Millionaire Tax, a
2-cent tax on the wealth of fortunes above $50 million, tackles this head on.
Under this tax, the top 0.1% – the wealthiest 75,000 Americans – would have to
pitch in two cents for every dollar of net worth above $50 million and three
cents for every dollar on net worth over $1 billion. With this version of the
Ultra-Millionaire Tax in place, the tax burden on the wealthiest households
would increase from 3.2% to 4.3% of total
wealth – better, but still below the 7.2% that the bottom 99% are projected to
pay.
Today, I’m going one step further. By asking
billionaires to pitch in six cents on each dollar of net worth above $1
billion, we can raise an additional $1 trillion in revenue and further close
the gap between what middle-class families pay as a percentage of their wealth
and what the top one-tenth of one percent pay.
Yes, billionaires will have to pay a little more, but they
will still likely pay less than what they would earn just from putting their
assets into an index fund and doing nothing. The average annual rate of return
of the S&P 500 has regularly topped 10%. And billionaires
have access to the kinds of fancy investment opportunities that can generate
even higher returns on average. Put it this way – should we ask billionaires to
pitch in an extra three cents on every dollar above $1 billion, or force
middle-class families to bear another $1 trillion in health care costs?
We can also change the way the government taxes investment
income for the top 1%. Today, taxes are only assessed on capital gains when securities are sold.
That means wealthy investors can put their money in the stock market, see it
grow, and not pay a dime in
taxes on those earnings unless or until it is taken out of the market. Under
the current system, they can then pass along those shares to their heirs when
they die and their heirs will be able to pay even less when
they choose to sell.
I’ve already proposed closing that loophole for how capital
gains are treated when shares are passed on to heirs. But we can go a step
further. Under a “mark-to-market” system for
the wealthiest 1% of households, we will tax capital gains income (excluding
retirement accounts) annually, rather than at the time of sale, and raise the
rates on capital gains to match the tax rates for labor income. Individuals
would still only pay taxes on gains and could use current losses to offset
future taxes.
Under this system, investment income will no longer be
treated differently than labor income for the top 1% of households.
Ultra-millionaires and billionaires won’t be able to earn income on giant
fortunes year after year without paying a penny in taxes. Andwe
can raise another $2 trillion over
ten years to pay for my Medicare for All plan.
IMMIGRATION REFORM
I support immigration reform that’s consistent with our
values, including a pathway to citizenship for undocumented immigrants and
expanded legal immigration consistent with my principles. That’s not only the
right thing to do – it also increases federal revenue we can dedicate to
Medicare for All as new people come into the system and pay taxes. Based on
CBO’s analysis of the 2013 comprehensive immigration reform bill, experts
project that immigration reform would generate an additional $400 billion in
direct federal revenue.
REINING IN DEFENSE SPENDING
Since the attacks of 9/11, the United States has
appropriated $2 trillion to fund
combat and counterterrorism operations around the world via the Overseas
Contingency Operations fund, or OCO. On average this spending has amounted
to $116 billion per
year – and in total, an amount equivalent to nearly 10 percent of all
federal discretionary spending over that same time period.
Republicans –
including the President’s current Chief of Staff – and Democrats alike
agree that OCO is a budget gimmick that masks the true impact of war spending.
The emergency supplemental funding mechanism was never intended to fund the
costs of long-scale, long-term operations outside of the normal appropriations
process. And in recent years, OCO has also been used to fund so-called “base”
requirements unrelated to the wars, outside of the Budget Control Act caps – in
effect acting as a slush fund for increased Pentagon spending. And as
everything from more F-35s to massive bombs never
used in combat have migrated into the OCO account, the Department of Defense
has been spared from having to prioritize or live
within its means. It’s not just bad budgetary practice – it’s wasteful
spending.
I’ve called out this
slush fund for what it is. I’ve also called for an end to endless
combat engagements in places like Afghanistan, Iraq, and Syria, and to
responsibly bring our combat troops home from these nations. These open-ended
commitments are not necessary to advance American foreign policy or
counterterrorism interests, their human cost has been staggering, and their
financial cost has created a drag on our economy by diverting money better
invested in critical domestic priorities.
I’ve also called to reduce defense spending overall.
The Pentagon budget will cost more this year than
everything else in the discretionary budget put together. That’s wrong, and
it’s unsustainable. We need to identify which programs actually benefit American
security in the 21st century, and which programs merely line the pockets of
defense contractors – then pull out a sharp knife and make some cuts.
As I have said repeatedly, under my Medicare for All plan,
costs will go up for the very wealthy and big corporations, and costs will go
down for middle-class families. I will not sign a bill that violates these
commitments. And as my plan to pay for Medicare for All makes clear, we can
meet these commitments without a tax increase on the middle class – and, in
fact, without any increase in income taxes at all.
America’s middle class is facing a crisis. For a generation,
wages have remained largely flat while family costs have exploded. I’ve spent
decades sounding the alarm about it. I’m running for President to fix it. That
means doing whatever we can to reduce the overall strain on family budgets.
Medicare for All can be a huge part of the solution. When
fully implemented, my approach to Medicare for All would mark one of the
greatest federal expansions of middle class wealth in our history. And
if Medicare for All can be financed without any new taxes on the middle class,
and instead by asking giant corporations, the wealthy, and the well-connected
to pay their fair share, that’s exactly what we should do.
ACHIEVING MEDICARE FOR ALL
Of course, moving to this kind of system will not be easy and
will not happen overnight. This is why every serious proposal for Medicare for
All contemplates a significant transition period.
In the weeks ahead, I will propose a transition plan that
will specifically address how I would use this time to begin providing
immediate financial relief to struggling families, rein in out-of-control
health care costs, increase coverage, and save lives. My transition plan will
take seriously and address substantively the concerns of unions, individuals
with private insurance, hospitals, people who work for private health insurers,
and medical professionals who worry about what a new system will mean for them.
It will also grapple directly with the entrenched political and economic
interests that would spend freely, as they havethroughout modern
American history, to influence politicians and
try to frighten the
American people into rejecting a plan that would save them thousands of dollars a year on
premiums and deductibles while making sure they can always see the health care
providers they need with false claims and scare tactics.
But there’s a reason former President Barack Obama has called Medicare for
All a good idea. There’s a reason the American people support it. It’s
because when it comes to the cost of health care, we are in the middle of a
full-blown crisis.
We are paying twice as much as
any other major nation for care – even as tens of millions lack
coverage, and even as family after family sees its finances destroyed by a
health issue. And the American people know that in the
long-term, a simple system that covers everybody, provides the care they need
when they need it, puts $11 trillion back in their pockets and uses all of the
public’s leverage to keep costs as low as possible is the best option for their
family budgets and for the health of their loved ones.
As President, I’ll fight to get it done.
Read the plan here
Read expert letter on cost estimate of Medicare for All here
Read expert letter on financing Medicare for All here
Calculator here
Amid
a sea of “Bernie” signs and chants of “We are the 99%” and “We will win”, Jane
Sanders, looked out over the massive crowd of 25,000 that overflowed
Queensbridge Park, beneath the Queensborough Bridge, onto the street, and said,
“Here are people from every background in the melting pot called New York. Most
of our ancestors came to America for a better life- mine from Ireland to escape
famine, poverty; Bernie’s from Poland escaping anti-Semitism, poverty.
“All believed they could have a better life. But in the last 40 years that
promise has eroded. Bernie plans to change that.” And, noting that this is his
first rally since his heart attack, she said to massive cheers, “Bernie is
back. He’s healthy and more than ready to continue his lifelong fight for
working people of America.”
Michael Moore: “This is not just about defeating Trump, but the
rotten system that gave us Trump’
Democracy,
said documentary filmmaker Michael Moore, is where “Everyone gets a seat at the
table, a slice of the pie and not fight for last crumbs. We don’t just need a
democratic politics, we need a democratic economy.”
Moore said, “The powers that be are very unhappy you’re here, that Bernie is
back. The pundits, the media [boo] are throwing everything out there to get
people to think differently:
“That Bernie is too old. Here’s what’s too old: the Electoral College, the
$7 minimum wage, women not being paid the same as men, thousands and thousands
of dollars of student debt, $10,000 deductible for health care, Super
Delegates, the fossil fuel industry – that’s what’s too old.
“It’s a gift we have 78-year-old American running for president. The
experience he has, what he has seen. He knows what a pay raise is, a pension –
look it up. What it looks like to defend against fascism and white supremacy,
to have the library open every day, what regulations are (Boeing). I’m glad
he’s 78.
“Health? We should be talking about the health of planet that’s dying [crowd
chants “Green New Deal”]; the health of kids in Flint Michigan, of 40 million
living in poverty, of young black males shot in back by police [chant Black
Lives Matter, Black Lives Count]. The only heart attack we should talk about is
the one Wall Street will have when Bernie wins.
“Next, that Bernie can’t win. He will win he has won 8 times to the House, 2
times to the Senate, 22 states in 2016 – almost half [chant “We will win.]. In
2016 [Democratic primary], Bernie won Michigan, Wisconsin, Minnesota. Of the 11
states that border Canada, Bernie won 10 (not NY) [boo] – we can fix that. Of
the 5 states that border the Pacific, he won 4; of 6 in New England, won 4;
Bernie won West Virginia – all 55 counties. According to a poll, he is #1 in
Nevada, a dead heat in Iowa, #1 in New Hampshire. He has raised more money from
more donors with the smallest amount.
“Why say Bernie can’t win? Because they are lying to the American people.
Bernie will win. [Chant, “We will win”]
“They say he can’t win because he is a [Democratic] socialist [yay!]. That’s
not going to fly. The American people have loved socialism for the last 70
years. Social Security, free public school, Medicare, Medicaid, fire department
– all are socialist.
“What they don’t want to do is tell the truth, what would happen if they
structured economic policies with democracy instead of capitalism. And this
isn’t capitalism of your great grandpa, this is a form of greed, selfishness so
that just few at the top succeed, the rest struggle paycheck to paycheck.
“Afraid taxes on rich will go up under Sanders? It was depressing during the
debate to watch Democrats go after Medicare for All. What would Franklin
Roosevelt say?
“They say we can’t afford it? How does Canada afford it? Every other
industrialized country has figured it out, why can’t we? They don’t want us to
figure it out.
“They say taxes will go up? That is part of the big lie – your taxes already
are up. We don’t call it a tax – in Canada, France, Finland they get free
health care, free or nearly free day care and college, but pay more in tax for
these things. The average American family pays $12,000 a year for child care,
$4000 in student loans, $6000 for deductibles, co-pays and premiums for health
care – too damn much – the average is $20,000/year but we don’t call it a tax.
“We are here in Queensbridge Park, Manhattan Island just across the river is
headquarters of corporate America [boo], corporate media [boo], Wall Street
[boo]
. So much misery has been visited on the American people from a half mile
away. It must stop.
“They must hear us at Goldman Sachs, Fox News, Trump Tower – the scene of
the crime.
“This [election] is not just about defeating Trump, but the rotten system
that gave us Trump…. beating Trump isn’t enough. We must crush Trump at
the polls, then fix the rotten corrupt economic system that gave us Trump.”
San Juan Mayor Cruz: “Move forward on the path of progressive agenda.
We are equal. We will win. We must win.”
Calling herself a “climate change survivor,” San Juan Mayor Carmen Yulín Cruz
Soto, attacked Trump for “killing us with inefficiency” that contributed to
3,000 Puerto Ricans dying after being smacked by back-to-back hurricanes.
“Why we have to win” she says is for Medicare-for-All, so no one has to
choose between groceries and insulin; to be able to afford college and life
after college, to “stand against those who earn $100 million and pay workers
starving wages; who take away women’s right to choose; the crime of separating
families at southern border; climate change.
“I am a climate change survivor. Climate change is real – 3000 Puerto Ricans
were killed because Trump Is a racist, xenophobic, paper throwing demagogue.” [Chant, “Lock him up.
Vote him out.”]
“The time is now to be fearless, relentless. I stand with Sanders – I respect
every other candidate but there is one name only who can get the job done. Be
united in one progressive voice, cross generations. Move forward on the path of
progressive agenda. We are equal. We will win. We must win.”
Nina Turner: “We must knock out Billionaire class that doesn’t
believe working people deserve a good life.”
National
co chair Nina Turner quoted Congresswoman Barbara Jordan who said American
people want an America as good as its promise. “That means an America where
people don’t die because have to ration insulin; hospitals are not closing;
where there is clean water, air, food; a justice system that doesn’t gun down
black folks in their houses.
“We need to clean up the criminal injustice system, Truth & Reconciliation
about the ravages of racism, a health care system not commodified. We need to
take care of Mother Earth.”
Alluding to the Democratic candidates, she said, “There are many copies but
only one original. We finally have somebody in our lifetime, his own special
interest is people of nation.
“We must knock out Billionaire class that doesn’t believe working people
deserve a good life.”
Congresswoman Alexandria Ocasio-Cortez: “We need a United States
truly, authentically operated, owned by working people.”
“We must bring revolution of working class to the ballot box of America,”
declared Congresswoman Alexandria Ocasio-Cortez. She prompted chants of “Green
New Deal,” saying, “Queensbridge Park is ground zero in the fight for public
housing and environmental justice.
“Last February I was working as a waitress in Manhattan, shoulder to
shoulder with undocumented workers who were putting in12 hour days with no
healthcare, not a living wage. We didn’t think we deserved it. That is the
script we tell working people: your inherent worth, value as human depends on
income another underpays. Turn around that basic language… We must change the
system that puts corporate profit ahead of all human and planetary costs.”
After her parents put all they had to buy a house, she said she learned from
an early age that “kids’ destiny determined by zipcode. Income inequality is a
fact of life of children.” Her father died of cancer when she was 18 and she
learned, “We all are one accident away from everything falling apart.
Sanders, she said, has fought for Planned Parenthood, for public education,
for CHIP, for single-payer health care, for gender rights, to end
“life-crushing” student debt.
“He didn’t do it because it was popular. He fought when it came at the
highest political cost in America.
“In 2016, he changed politics in America. We now have one of the best
Democratic fields – much because of Sanders.
“I’m in Congress today but one year ago I was a sexually harassed waitress.
This freshman class in overwhelming numbers rejected corporate money – thanks
to Bernie – endorsed Medicare for All, sees the climate crisis as an
existential threat.
“[In Congress] it is no joke to stand up against corporate power and
establishment interests. Arms are twisted, political pressure psychological and
otherwise applied to make you abandon the working class.
“I have come to appreciate the nonstop advocacy of Sanders. It’s not just
what he fights for but how: mass mobilization of the working class at the
ballot box, a movement (against) racism, classism of Hyde Amendment,
imperialist and colonial histories that lead to endless war and immigration
crisis.
“NYCHA is underfunded by $30 billion –that is not an accident, but an
outcome of system that devalues poor, Logic that got us into this won’t get us
out.”
Senator Amy Klobuchar,left, on stage in Houston for the third Democratic Debate, hosted by ABC News.
Senator Amy Klobuchar had her best moments in the third
Democratic Debate, Sept. 12, in addressing health care and drawing the
distinction between Senator Bernie Sanders’ Medicare-for-All solution in the
quest, shared by all the Democratic candidates, of universal health care at an
affordable cost, health care as a right, not a privilege.
This is from the Klobuchar campaign:
MINNEAPOLIS, MN — Senator Amy Klobuchar has been a leader in the Senate to lower the cost of prescription drugs, expand access to affordable health care and protect reproductive rights. She was the first candidate in this race to release a comprehensive plan to combat addiction and prioritize mental health — two issues she’s championed her entire career.
Senator Klobuchar supports:
Universal health care for all Americans, and she
believes the quickest way to get there is through a public option that
expands Medicare or Medicaid.
Changes to the Affordable Care Act to help bring
down costs to consumers including providing cost-sharing reductions, making it
easier for states to put reinsurance in place, and continuing to implement
delivery system reform.
Lifting the ban on Medicare negotiations for
prescription drugs, allowing personal importation of safe drugs from countries
like Canada, and stopping pharmaceutical companies from blocking less-expensive generics.
Taking on mental health and addiction by launching
new prevention and early intervention initiatives, expanding access to treatment,
and giving Americans a path to sustainable recovery because she believes
everyone has the right — and the opportunity — to receive effective,
professional treatment and help.
Stopping the concerted attack to undermine and
eliminate a woman’s right to make her own health care decisions. She believes
recent bans in states are dangerous, they are unconstitutional, and they are
out of step with the majority of Americans. Amy will continue working to
protect the health and lives of women across the country.
Immediately suspend the Trump Administration’s
efforts to eliminate the Affordable Care Act’s protections for people with
pre-existing conditions.
Immediately allow for the safe importation of
prescription drugs from countries like Canada.
Expand VA health benefits for women veterans and
their babies.
Prioritize mental health and addiction.
End “pay for delay” agreements that increase the
cost of prescription drugs.
Propose legislation to get us to universal health
care.
Develop best models of care to address disparities
in maternal and infant mortality and address the shortage of maternity care
health professional in underserved rural and urban areas.
Stop Trump sabotage of the ACA by ending workarounds
that allow states to raise premiums for sicker people and shift ACA premium
subsidies away from lower-income enrollees.
End the sale of junk insurance policies that
eliminate existing protections for consumers.
End anticompetitive practices that increase the
price of prescription drugs.
Encourage reinsurance programs.
Expand Medicaid reimbursement for people receiving
mental health or substance use treatment.
Ensure
funding for Planned Parenthood, end the gag rule, and restore the Title X
program.
Expand investments in veterans telehealth
services.
Invest in the Veterans Health Administration.
Reassess the granting of Medicaid waivers, including
states that have privatized Medicaid.
Direct the Department of Defense and VA to track
servicemembers and veterans exposed to toxic chemicals.
Direct the Department of Health and Human Services
to consider VHA facilities when designating Health Professional Shortage
Areas.
Strengthen the National Science Foundation and the
National Institutes of Health.
Invest in Alzheimer’s research.
Prioritize health care delivery system reform to
reduce health care costs.
Expand the open enrollment period for health
insurance under the Affordable Care Act so more people can get insurance
coverage.
WASHINGTON – U.S. Senator Bernie Sanders, running to be the Democratic nominee for president, on July 17 delivered a major address on Medicare for All, coinciding with the 54th anniversary of Medicare being signed into law. In his remarks, Sanders outlined his plan to make health care a human right for all Americans. Here is highlighted transcript of remarks as they were prepared for delivery: – Karen Rubin, News & Photo Features
Thank you all very
much for being here to discuss one of the major crises facing our country.
Let me also thank the dozens of organizations throughout America who
support Medicare for All and the tens of thousands of doctors, nurses and other
health professionals who support my legislation. Let me thank the 14
Senate co-sponsors that we have on this legislation and the 118 Members of the
House who support similar legislation. And mostly, let me thank the
American people who by the millions understand, as I do, that health care is a
human right, not a privilege.
Together, we will end
the international embarrassment of the United States being the only major
country on earth that does not guarantee health care to all of its citizens.
It is not acceptable to
me, nor to the American people, that some 87
million people today are either uninsured or underinsured.
It is not acceptable
to me that we end up spending almost
twice as much as any other major country on health care, while our life expectancy continues to decline
and our healthcare outcomes lag behind many other countries.
Frankly, I am sick and
tired of talking to doctors who tell me about the patients who died because
they were uninsured or underinsured, and walked into the doctor’s office when
it was too late. And we are talking about over 30,000 Americans who die every year because they are uninsured or
under-insured. What a tragedy.
I am sick and tired of
seeing working class families and small
businesses pay far more for healthcare than they can afford, and 530,000 Americans declare bankruptcy each
year because they cannot pay off the outrageous cost of a medical emergency
or a hospital stay. Families should not be driven into financial ruin
because someone in the family became seriously ill. How insane is that?
I am sick and tired of
hearing from Americans who lost loved ones because they could not afford the unbelievably high cost of prescription drugs, or
hearing from constituents who are forced to cut their pills in half due to the
cost.
In fact, later this
month, I will be travelling from Detroit, Michigan to Windsor, Ontario with a
busload of Americans who have diabetes in order to purchase insulin in Canada
at one-tenth of the price that they pay in America.
I am sick and tired of
talking with people who are struggling with mental illness but cannot afford the mental health counseling they
desperately need.
I am tired of talking
to people who have teeth that are rotting in their mouths, but cannot afford the high cost of dental care.
Let me be very honest
and tell you that, in my view, the
current debate over Medicare for All really has nothing to do with healthcare.
It has everything to do with greed and the desire of the healthcare
industry to maintain a system which fails the average American, but which makes
the industry tens and tens of billions of dollars every year in profit.
It is about whether we
maintain a dysfunctional system which
allows the big drug and health insurance companies to make over $100 billion in
profits last year, while the top CEOs in that industry made $2.6 billion in
total compensation – all the while 1 out of 5 Americans cannot afford the
prescription drugs their doctors prescribe.
It’s about whether we
maintain a system in which the CEO of the Aetna insurance company, Mr. Mark
Bertolini, received a golden parachute worth nearly $500 million after his
company merged with CVS Health, while elderly people lack the resources to
purchase a hearing aid.
It’s about whether we
maintain a system that allows the former CEO
from Gilead (John Martin) to become a billionaire by charging $1,000 a pill for
a hepatitis c drug called Sovaldi that costs a dollar to manufacture.
Let us make no mistake
about it. The struggle that we are
now undertaking, to guarantee health care to all Americans as a right and to
substantially lower the cost of prescription drugs, will be opposed by some of
the most powerful forces in America – entities that have unlimited amounts of
money. We’re talking about the insurance companies, the drug companies,
private hospitals, medical equipment suppliers, Wall Street and other powerful
entities.
Let me make a
prediction. In order to defeat the Medicare for All movement, powerful special
interests will be spending millions on 30 second television ads, full page
magazine ads, and corporate-sponsored “studies” to frighten the American people
about Medicare for All – which is exactly what happened before the passage of
Medicare in the 1960s. They failed then and they’re going to fail now.
And let me give you an
example of the kind of money and power we are talking about.
Over the last 20 years, the insurance industry
and pharmaceutical companies have spent more than $330 million in campaign
contributions and over $4 billion in lobbying to get Congress to do its
bidding.
The pharmaceutical industry alone has hired
some 1,200 lobbyists – including the former leadership of both political
parties.
I find it quite
interesting that Billy Tauzin, the
Republican Congressman who wrote the bill to prevent Medicare from negotiating
for lower drug prices and then went on to become the President and CEO of
Pharma, received over $11.6 million in compensation in 2010.
That’s how business is done in Washington. Well, I have a different vision of what
a rational healthcare system is all about. Instead of massive profits for the drug companies, the insurance
companies and Wall Street, we must provide a healthcare system that provides
quality healthcare to all in a cost effective way.
And that is exactly what Medicare for All does.
Under this
legislation, every family in America
would receive comprehensive coverage, and middle-class families would save
thousands of dollars a year by eliminating their private insurance costs as we
move to a publicly funded program.
The transition to the Medicare for All program
would take place over four years. In the first year, benefits to older people
would be expanded to include dental care, vision coverage and hearing aids, and
the eligibility age for Medicare would be lowered to 55. All children under the
age of 18 would also be covered. In the second year, the eligibility age would
be lowered to 45 and in the third year to 35. By the fourth year, every man,
woman and child in the country would be covered by Medicare for All.
Medicare for All will reduce – let me repeat,
reduce — overall health care spending while lowering the number of uninsured
and underinsured people in this country to zero.
We accomplish this
because Medicare for All creates a
system of health care insurance that isn’t designed to generate profits for
insurance and drug companies — it will be a system focused on delivering actual health care. It will save lives, save money, and end the
frustration of endless paperwork, denials, and desperate fights with an
insurance company to cover medically-necessary medications and procedures.
Medicare for All will
fully eliminate health insurance premiums, deductibles and co-payments. Make no
mistake about it: These are nothing less than taxes on the middle class.
And when we do that, the
average middle class family will save an estimated $3,000 each and every year.
Further, unlike the
current dysfunctional system, Medicare for All allows people the freedom to
choose any doctor, clinic, and hospital without worrying about whether their provider is in-network or
not. People will be able to make
the health care choices that are best for themselves and their families without
some insurance bureaucrat telling them which providers they can see or not
see. Medicare for All is at the end of the day empowering patients and health
care providers.
In addition, a
Medicare for All system will allow us to
address the serious problem of medically underserved areas.
Just to demonstrate
how absurd our health care system is, I was in Philadelphia two days ago
rallying with the people of that city to try to stop the closure of Hahnemann
University Hospital, an important, safety net hospital in that community.
Why do the owners want to close this hospital? Because they can make more
money redeveloping that property into condominiums and hotels.
Let me address some of
the half-truths, misinformation, and, in some cases, outright lies that people
may be hearing about Medicare for All.
Medicare for All
critics tell us that Americans just love their private health insurance
companies. We heard this most recently from UnitedHealth CEO David Wichmann,
who by the way, made $83 million in 2017 and who said Medicare for All would
“destabilize the nation’s health system.”
But let’s remember: the current system is already disrupting
and destabilizing millions of people’s lives. In the current system, 50 million
Americans every year lose their existing health insurance when their employer
changes insurer, when they change jobs, or when they cannot afford their current
plan. For many of them, they will no longer be able to see the doctor they have
relied on for years. For others, important treatments for long-term
conditions or disabilities will be changed or stopped altogether.
Here is the simple
truth. The American people do not like their private health insurance
companies. In fact private health insurance companies are quite unpopular.
What the American people do like are their doctors, nurses and other
health care providers.
While our opponents
claim that Medicare for All is too expensive, the reality is that it is much more cost effective than our
current system.
The Center for
Medicare and Medicaid Services estimates that, if we do not change the system, this country will be spending $50
trillion over the next ten years –19.4 percent of our nation’s GDP.
This is unsustainable and will be incredibly harmful to the people of our
country, to the business community, and to the entire economy.
And the reason why we spend so much is obvious. It
is not just the huge profits in the insurance industry and the pharmaceutical
industry, but it is the incredible and wasteful bureaucratic maze developed by
thousands of different healthcare plans. Today, hospitals and doctors
must deal with patients who have different deductibles, different co-payments,
different networks of coverage, and different coverage for pharmaceuticals, or
no insurance at all. All of this is not only driving doctors and nurses
and hospital administrators to distraction, but it is wasting
up to $500 billion a year on unnecessary administrative costs.
Unlike our current
system, there is broad consensus – from conservative to progressive economists
– that Medicare for All would result in substantial savings to the American
people. Two of the most recent studies on this issue have estimated that Medicare
for All would save the American people between $2 trillion and $5 trillion over
a 10-year period.
Let us be clear, the
fight against Medicare for All today is not a new development. Powerful
special interests have always opposed healthcare programs that work for the
people and not for corporate interests.
Let us not forget that
when President Harry Truman first proposed a program guaranteeing health care
to seniors that idea was billed as radical, “un-American,” and an attack on
basic freedom. And because of that assault, the idea stalled in Congress for
years — until voters made their voices heard.
In 1960, America
elected John F. Kennedy after he campaigned in support of Truman’s idea. That
election prompted serious work on universal health care bill, and Kennedy at
the time noted that “what we are now talking about doing, most of the countries
of Europe did years ago.”
Finally, following the
1964 Democratic election landslide, the new Congress was able to pass what is
now known as Medicare despite intense opposition from the health insurance
industry and the pharmaceutical companies.
More than a
half-century after that achievement, the time is now to go forward. The
time is now to expand Medicare to every man, woman and child in this
country.
Let us be very clear.
When it comes to health care, the insurance and drug industries have been
able to control the political process.
If we are going to break the stranglehold of
corporate interests over the health care needs of the American people, we have
got to confront a Washington culture that is corrupt, that puts profits before
people.
That is why I am
calling on every Democratic candidate in this election to join me in rejecting
money from the insurance and drug industries. That means not accepting
donations over $200 from health insurance or pharmaceutical company PACs,
lobbyists or executives. Candidates who are not willing to take that pledge
should explain to the American people why those corporate interests believe
their campaigns are a good investment.
Of course, President Trump should do the same but I am not going
to even waste my breath suggesting that he will. His efforts to throw 32
million people off their health insurance to have it replaced with junk
insurance shows exactly what side he is on.
Finally, let me say,
eliminating health insurance and drug company money from the Democratic primary
won’t solve all the problems, but it is an important step forward. Now is the
time to tell the health care industry that your profits are not more important
than the lives of the American people.
Vice
President Joe Biden, in the race for the Democratic nomination for President,
has staked out a position on improving on the Affordable Care Act (Obamacare)
as his solution to providing universal healthcare – essentially, enabling people keep their
private insurance but creating a new public option. That is more moderate than
the Democrats like Bernie Sanders and Elizabeth Warren who want a more extreme
Medicare for All that replaces private insurance (though it is unlikely that
there will not still be a market for supplemental private insurance, just as
there is now for Medicare). Here, is the Biden campaign’s description and
rationale for Biden’s plan to protect and build upon the Affordable Care Act: – Karen Rubin, News&
Photo Features
On March 23, 2010, President Obama signed the
Affordable Care Act into law, with Vice President Biden standing by his side,
and made history. It was a victory 100 years in the making. It was the
conclusion of a tough fight that required taking on Republicans, special
interests, and the status quo to do what’s right. But the Obama-Biden
Administration got it done.
But, every day over the past nine years, the Affordable Care Act has been under
relentless attack.
Immediately after its passage, Congressional Republicans began trying again and
again to repeal it. Following the lead of President
Trump, Republicans in Congress have only doubled down on this
approach since January 2017. And, since repeal through Congress has not been
working, President Trump has been unilaterally doing everything he can to
sabotage the Affordable Care Act. Now, the Trump Administration is trying to
get the entire law – including protections for people with pre-existing
conditions – struck down in court.
As president, Biden will protect the Affordable Care Act from
these continued attacks. He opposes every effort to get rid of this historic
law – including efforts by Republicans, and efforts by Democrats. Instead of
starting from scratch and getting rid of private insurance, he has a plan
to build on the Affordable Care Act by giving Americans more choice, reducing
health care costs, and making our health care system less complex
to navigate.
For Biden, this is personal. He believes that every American has a right to the
peace of mind that comes with knowing they have access to affordable, quality
health care. He knows that no one in this country should have to lay in bed at
night staring at the ceiling wondering, “what will I do if she gets breast cancer?”
or “if he has a heart attack?” “Will I go bankrupt?” He knows there is no peace
of mind if you cannot afford to care for a sick child or a family member
because of a pre-existing condition, because you’ve reached a point where your
health insurer says “no more,” or because you have to make a decision between
putting food on the table and going to the doctor or filling a prescription.
In the coming months, Joe Biden will build on today’s plan by rolling out his
proposals to tackle some of our greatest public health challenges – from
reducing gun violence to curing devastating diseases as we know them like
cancer, Alzheimer’s, diabetes, and addiction.
I. GIVE EVERY AMERICAN ACCESS TO AFFORDABLE HEALTH INSURANCE
From the time right before the Affordable Care Act’s key coverage-related
policies went into effect to the last full year of the Obama-Biden
Administration, 2016, the number of Americans lacking health insurance fell
from 44 million to 27 million –
an almost 40% drop. But President Trump’s persistent efforts to sabotage
Obamacare through executive action, after failing in his efforts to repeal it
through Congress, have started to reverse this progress. Since 2016, the number
of uninsured Americans has increased by
roughly 1.4 million.
As president, Biden will stop this reversal of the progress made by Obamacare.
And he won’t stop there. He’ll also build on the Affordable Care Act with a
plan to insure more than an estimated 97% of Americans. Here’s how:
Giving Americans a new choice, a public
health insurance option like Medicare. If your insurance
company isn’t doing right by you, you should have another, better choice.
Whether you’re covered through your employer, buying your insurance on your
own, or going without coverage altogether, the Biden Plan will give you the
choice to purchase a public health insurance option like Medicare. As in
Medicare, the Biden public option will reduce costs for patients by negotiating
lower prices from hospitals and other health care providers. It also will better coordinate among
all of a patient’s doctors to improve the efficacy and quality of their care,
and cover primary care without any co-payments. And it will bring relief to
small businesses struggling to afford coverage for their employees.
Increasing the value of tax credits to
lower premiums and extend coverage to more working Americans. Today,
families that make between 100% and 400% of the
federal poverty level may receive a tax credit to reduce how
much they have to pay for health insurance on the individual marketplace. The
dollar amount of the financial assistance is calculated to ensure each family
does not have to pay more than a certain percentage of their
income on a silver (medium generosity) plan. But, these shares of
income are too high and silver plans’ deductibles are too high. Additionally,
many families making more than 400% of the federal poverty level (about $50,000 for a single person
and $100,000 for a family of four), and thus not qualifying for
financial assistance, still struggle to afford health insurance. The Biden Plan
will help middle class families by eliminating the 400% income cap on tax
credit eligibility and lowering the limit on the cost of coverage from 9.86% of
income to 8.5%. This means that no family buying insurance on the individual
marketplace, regardless of income, will have to spend more than 8.5% of their
income on health insurance. Additionally, the Biden Plan will increase the size
of tax credits by calculating them based on the
cost of a more generous gold plan, rather than a silver plan. This
will give more families the ability to afford more generous coverage, with
lower deductibles and out-of-pocket costs.
Expanding coverage to low-income
Americans. Access to affordable health insurance
shouldn’t depend on your state’s politics. But today, state politics is getting
in the way of coverage for millions of low-income Americans. Governors and
state legislatures in 14 states have
refused to take up the Affordable Care Act’s expansion of Medicaid eligibility,
denying access to Medicaid for an estimated 4.9 million adults.
Biden’s plan will ensure these individuals get covered by offering premium-free
access to the public option for those 4.9 million individuals who would be
eligible for Medicaid but for their state’s inaction, and making sure their
public option covers the full scope of Medicaid benefits. States that have
already expanded Medicaid will have the choice of moving the expansion
population to the premium-free public option as long as the states continue to
pay their current share of the cost of covering those individuals.
Additionally, Biden will ensure people making below 138% of the federal poverty
level get covered. He’ll do this by automatically enrolling these individuals
when they interact with certain institutions (such as public schools) or other
programs for low-income populations (such as SNAP).
II. PROVIDE THE PEACE OF MIND OF
AFFORDABLE, QUALITY HEALTH CARE AND A LESS COMPLEX HEALTH CARE SYSTEM
Today, even for people with health insurance, our health care system is too
expensive and too hard to navigate. The Biden Plan will not only provide
coverage for uninsured Americans, it will also make health care more affordable
and less complex for all.
The plan’s elements described above will help reduce the cost of health
insurance and health care for those already insured in the following ways:
All Americans will have a new, more
affordable option. The public option, like Medicare,
will negotiate prices with providers, providing a more affordable option for
many Americans who today find their health insurance too expensive.
Middle class families will get a premium
tax credit to help them pay for coverage. For
example, take a family of four with an income of $110,000 per year. If they
currently get insurance on the individual marketplace, because their premium
will now be capped at 8.5% of their income, under the Biden Plan they will
save an estimated $750 per month on
insurance alone. That’s cutting their premiums almost in half. If a family is
covered by their employer but can get a better deal with the 8.5% premium cap,
they can switch to a plan on the individual marketplace, too.
Premium tax credits will be calculated
to help more families afford better coverage with lower deductibles. Because
the premium tax credits will now be calculated based on the price of a more
generous gold plan, families will be able to purchase a plan with a lower
deductible and lower out-of-pocket spending. That means many families will see
their overall annual health care spending go down.
The Biden Plan has several additional proposals
aimed directly at cutting the cost of health care and making the health care
system less complex to navigate. The Biden Plan will:
Stop “surprise billing.” Consumers
trying to lower their health care spending often try to choose an in-network
provider. But sometimes patients are unaware they are receiving care from an
out-of-network provider and a big, surprise bill. “Surprise medical billing”
could occur, for example, if you go to an in-network hospital but don’t realize
a specialist at that hospital is not part of your health plan. The Biden Plan
will bar health care providers from charging patients out-of-network rates when
the patient doesn’t have control over which provider the patient sees (for
example, during a hospitalization).
Tackle market concentration across our
health care system. The concentration of market power
in the hands of a few corporations is occurring throughout our health care system,
and this lack of competition is driving up prices for consumers.
The Biden Administration will aggressively use its existing antitrust authority
to address this problem.
Lower costs and improve health outcomes
by partnering with the health care workforce. The Biden
Administration will partner with health care workers and accelerate the testing
and deployment of innovative solutions that improve quality of care and
increase wages for low-wage health care workers, like home care workers.
III. STAND UP TO ABUSE OF POWER BY
PRESCRIPTION DRUG CORPORATIONS
Too many Americans cannot afford their prescription drugs, and prescription
drug corporations are profiteering off of the pocketbooks of sick individuals.
The Biden Plan will put a stop to runaway drug prices and the profiteering of
the drug industry by:
Repealing the outrageous exception
allowing drug corporations to avoid negotiating with Medicare over drug prices. Because
Medicare covers so many Americans, it has significant leverage to negotiate
lower prices for its beneficiaries. And it does so for hospitals and other
providers participating in the program, but not drug manufacturers. Drug
manufacturers not facing any competition, therefore, can charge whatever price
they choose to set. There’s no justification for this except the power of
prescription drug lobbying. The Biden Plan will repeal the existing law
explicitly barring Medicare from negotiating lower prices with drug
corporations.
Limiting launch prices for drugs that
face no competition and are being abusively priced by manufacturers. Through
his work on the Cancer Moonshot, Biden understands that the future of
pharmacological interventions is not traditional chemical drugs but specialized
biotech drugs that will have little to no competition to keep prices in check.
Without competition, we need a new approach for keeping the prices of these
drugs down. For these cases where new specialty drugs without competition are
being launched, under the Biden Plan the Secretary of Health and Human Services
will establish an independent review board to assess their value. The board
will recommend a reasonable price, based on the average price in other countries
(a process called external reference pricing)
or, if the drug is entering the U.S. market first, based on an evaluation by
the independent board members. This reasonable price will be the rate Medicare
and the public option will pay. In addition, the Biden Plan will allow private
plans participating in the individual marketplace to access a similar rate.
Limiting price increases for all brand,
biotech, and abusively priced generic drugs to inflation. As
a condition of participation in the Medicare program and public option, all
brand, biotech, and abusively priced generic drugs will be prohibited from
increasing their prices more than the general inflation rate. The Biden Plan
will also impose a tax penalty on drug manufacturers that increase the costs of
their brand, biotech, or abusively priced generic over the general inflation
rate.
Allowing consumers to buy prescription
drugs from other countries. To create more competition
for U.S. drug corporations, the Biden Plan will allow consumers to import
prescription drugs from other countries, as long as the U.S. Department of
Health and Human Services has certified that those drugs are safe.
Improving the supply of quality
generics. Generics help reduce health care spending, but
brand drug corporations have succeeded in preserving a number of strategies to
help them delay the entrance of a generic into the market even after the patent
has expired. The Biden Plan supports numerous proposals to accelerate the
development of safe generics, such as Senator Patrick Leahy’s proposal to
make sure generic manufacturers have access to a sample.
IV. ENSURE HEALTH CARE IS A RIGHT FOR
ALL, NOT A PRIVILEGE FOR JUST A FEW
Joe Biden believes that every American – regardless of gender, race, income,
sexual orientation, or zip code – should have access to affordable and quality
health care. Yet racism, sexism, homophobia, transphobia, and other forms of
discrimination permeate our health care system just as in every other part of
society. As president, Biden will be a champion for improving access to health
care and the health of all by:
Expanding access to contraception and
protect the constitutional right to an abortion. The
Affordable Care Act made historic progress by ensuring access to free preventive care, including
contraception. The Biden Plan will build on that progress. Vice
President Biden supports repealing the Hyde Amendment because health care is a
right that should not be dependent on one’s zip code or income. And, the public
option will cover contraception and a woman’s constitutional right to choose.
In addition, the Biden Plan will:
1) Reverse the Trump Administration and states’
all-out assault on women’s right to choose. As president, Biden will work to
codify Roe v. Wade, and
his Justice Department will do everything in its power to stop the rash of
state laws that so blatantly violate the constitutional right to an abortion,
such as so-called TRAP laws, parental
notification requirements, mandatory waiting periods, and ultrasound
requirements.
2) Restore federal funding for Planned Parenthood.
The Obama-Biden administration fought Republican attacks on funding for Planned
Parenthood again and again. As president, Biden will reissue guidance specifying
that states cannot refuse Medicaid funding for Planned Parenthood and other
providers that refer for abortions or provide related information and reverse
the Trump Administration’s rule preventing
Planned Parenthood and certain other family planning programs from obtaining
Title X funds.
3) Just as the Obama-Biden Administration did, President Biden
will rescind the Mexico City Policy (also referred to as the global gag rule) that
President Trump reinstated and
expanded. This rule currently bars the U.S. federal government from supporting
important global health efforts – including for malaria and HIV/AIDS – in
developing countries simply because the organizations providing that aid also
offer information on abortion services.
Reducing our unacceptably high maternal
mortality rate, which especially impacts people of color. Compared
to other developed nations, the U.S. has the highest rate of
deaths related to pregnancy and childbirth, and we are the only country
experiencing an increase in this death rate. This problem is especially
prevalent among black women, who experience a death rate from complications
related to pregnancy that is more than three times higher than
the rate for non-Hispanic white women. California came up with a strategy
that halved the state’s
maternal death rate. As president, Biden will take this strategy nationwide.
Defending health care protections for
all, regardless of gender, gender identity, or sexual orientation. Before
the Affordable Care Act, insurance companies could increase premiums merely due
to someone’s gender, sexual orientation, or gender identity. Further, insurance
companies could increase premiums or deny coverage altogether due to someone’s HIV status. Yet,
President Trump is trying to walk back this progress. For example, he has proposed to once
again allow health care providers and insurance companies to discriminate based
on a patient’s gender identity or abortion history. President Biden will defend
the rights of all people – regardless of gender, sexual orientation, gender
identity – to have access to quality, affordable health care free from
discrimination.
Doubling America’s investment in
community health centers. Community health centers
provide primary, prenatal, and other important care to underserved populations.
The Biden Plan will double the federal investment in these centers, expanding
access to high quality health care for the populations that need it most.
In the months ahead, Biden will put forward
additional plans to tackle health challenges affecting specific communities,
including access to health care in rural communities, gun violence, and opioid
addiction.
SUPPORTING HEALTH, NOT REWARDING
WEALTH
Joe Biden believes in rewarding work, not just wealth – and investing in
hard-working Americans’ health, not protecting the most privileged Americans’
wealth. Warren Buffett said it best when he stated that he should not pay a
lower tax rate than his secretary.
The Biden Plan will make health care a right by getting rid of capital gains
tax loopholes for the super wealthy. Today, the very wealthy pay a tax rate of
just 20% on long-term capital gains. According to the Joint Committee on
Taxation, the capital gains and dividends exclusion is the second largest tax
expenditure in the entire tax code: $127 billion in fiscal year 2019
alone. As President, Biden will roll back the Trump rate cut for the
very wealthy and restore the 39.6% top rate he helped restore when he negotiated an end to the Bush
tax cuts for the wealthy in 2012.
Biden’s capital gains reform will close the loopholes that allow the super
wealthy to avoid taxes on capital gains altogether. The Biden plan will assure
those making over $1 million will pay the top rate on capital gains, doubling
the capital gains tax rate on the super wealthy.
WATCH: Joe Biden
talks more about the need to build on and protect ACA in THIS new video.